Chinese Medical Sciences Journal ›› 2017, Vol. 32 ›› Issue (3): 161-170.doi: 10.24920/J1001-9294.2017.023
中国老年患者经桡动脉与股动脉介入治疗比较
金辰†, 徐奕†, 乔树宾, 唐欣然, 吴永健, 颜红兵, 窦克非, 徐波, 杨进刚, 杨跃进*( )
)
- 国家心血管病中心,中国医学科学院 北京协和医学院 阜外医院,北京 100037
-
收稿日期:2016-12-07出版日期:2017-09-27发布日期:2017-09-27 -
通讯作者:金辰,徐奕,杨跃进 E-mail:yangyjfw@126.com
Transradial Versus Transfemoral Approach for Percutaneous Coronary Intervention in Elderly Patients in China: A Retrospective Analysis
Jin Chen?, Xu Yi?, Qiao Shu-bin, Tang Xin-ran, Wu Yong-jian, Yan Hong-bing, Dou Ke-fei, Xu Bo, Yang Jin-gang, Yang Yue-jin*()
- State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, National Center of Cardiovascular Diseases, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing 100037, China
-
Received:2016-12-07Published:2017-09-27Online:2017-09-27 -
Contact:Jin Chen,Xu Yi,Yang Yue-jin E-mail:yangyjfw@126.com
摘要:
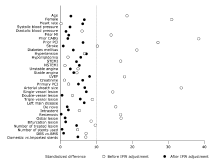
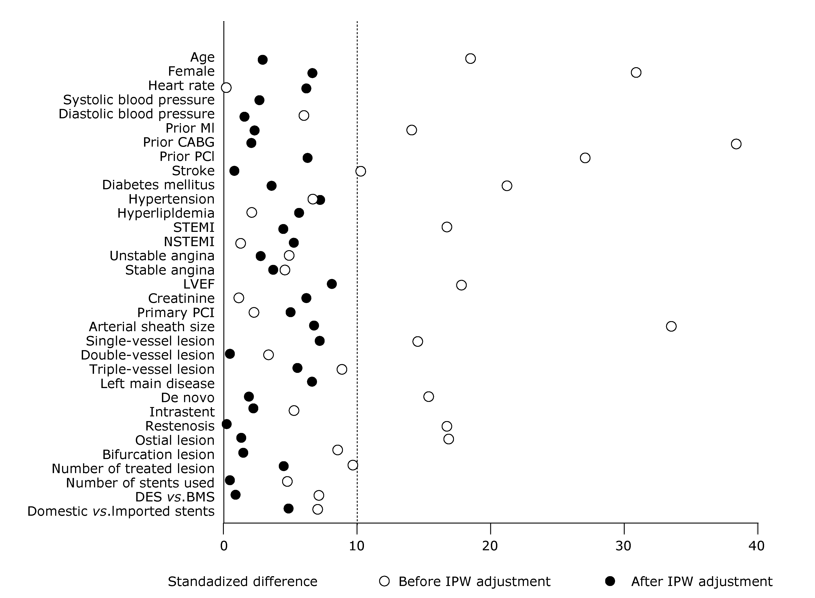
目的 从院内费用和临床结果两方面对65岁以上老年患者经桡动脉与股动脉路径行经皮冠状动脉介入治疗(percutaneous coronary intervention,PCI)进行比较和评价,为老年患者介入路径选择提供临床和卫生经济学依据。 方法 本研究为回顾性研究,共纳入阜外医院2010年1月1日至2010年12月31日收治的1229例年龄>65岁的PCI病例。其中,经桡动脉路径介入治疗(transradial intervention,TRI)1033例,经股动脉路径介入治疗(transfemoral intervention,TFI)196例。研究使用倾向性评分的逆概率加权法(inverse probability weighting,IPW)对两种路径的患者院内费用和临床结局进行了比较。依据出血学术研究联合会标准,对出血并发症及主要不良心血管事件(包括院内全因死亡、心肌梗死、住院期间再次血运重建及BARC分级≥3)进行了比较。结果 与TFI组相比,TRI组患者平均年龄较低,女性患者所占比例较低,且既往心肌梗死、既往冠状动脉旁路移植术史、既往PCI及既往卒中病史均较少。造影结果提示TRI组患者单支病变比例较高,而开口病变比例则较低。IPW调整后,TRI组患者的院内费用明显低于TFI组,差值为CNY7495(95%CI:4419-10420,P<0.0001),造成住院费用差异的主要原因是TRI组患者PCI术中花费较低。IPW调整后TRI组患者住院时间较短(差值=1.9 d,95%CI:1.1-2.7,P<0.0001),且主要不良心血管事件较少(OR=0.47,95%CI:0.31-0.73,P<0.001)。IPW调整前后,两组患者出血并发症的差异在无统计学意义(P>0.05)。结论 与股动脉路径PCI相比,桡动脉路径可降低65岁以上老年患者院内费用,缩短住院时间,减少主要不良心血管事件的发生。
引用本文
Jin Chen, Xu Yi, Qiao Shu-bin, Tang Xin-ran, Wu Yong-jian, Yan Hong-bing, Dou Ke-fei, Xu Bo, Yang Jin-gang, Yang Yue-jin. Transradial Versus Transfemoral Approach for Percutaneous Coronary Intervention in Elderly Patients in China: A Retrospective Analysis[J].Chinese Medical Sciences Journal, 2017, 32(3): 161-170.
"
| Characteristics | TRI group | TFI group | Standardized difference |
|---|---|---|---|
| n | 1033 | 96 | 18.5 |
| Age§ (yrs) | 71.0±8.4 | 71.7±3.9 | |
| Female [n (%)] | 361 (34.9) | 98 (50.0) | 30.8 |
| Medical history | |||
| Myocardial infarction [n (%)] | 174 (16.8) | 44 (22.4) | 14.1 |
| Prior CABG [n (%)] | 12 (1.2) | 19 (9.7) | 38.3 |
| Prior PCI [n (%)] | 179 (17.3) | 56 (28.6) | 27.0 |
| Stroke [n (%)] | 107 (10.4) | 27 (13.8) | 10.5 |
| Diabetes mellitus [n (%)] | 278 (26.9) | 72 (36.7) | 21.2 |
| Hypertension [n (%)] | 711 (68.8) | 141 (71.9) | 6.8 |
| Hyperlipidemia [n (%)] | 623 (60.3) | 110 (59.2) | 2.3 |
| Diagnosis | |||
| STEMI [n (%)] | 131 (12.7) | 15 (7.7) | 16.7 |
| NSTEMI [n (%)] | 45 (4.4) | 8 (4.1) | 1.4 |
| Unstable angina [n (%)] | 554 (53.6) | 110 (56.1) | 5.0 |
| Stable angina [n (%)] | 274 (26.5) | 56 (28.6) | 4.6 |
| Vital signs | |||
| Heart rate§ (bpm) | 69.1±10.6 | 69.1±8.7 | 0.1 |
| Systolic blood pressure§ (mm Hg) | 132.2±17.8 | 132.7±18.8 | 2.6 |
| Diastolic blood pressure§ (mm Hg) | 77.3±24.0 | 76.2±9.9 | 6.0 |
| LVEF§ (%) | 62.2±7.6 | 60.8±7.9 | 17.9 |
| Creatinine§ (μmol/L) | 84.4±20.7 | 84.1±21.4 | 1.2 |
"
| Characteristics | TRI group | TFI group | Standardized difference |
|---|---|---|---|
| n | 1033 | 196 | |
| Artery sheath size§(F) | 6.0±0.2 | 6.1±0.3 | 33.5 |
| Diseased coronary vessels | 978 | 171 | |
| Single vessel [n (%)] | 236 (24.1) | 31 (18.1) | 14.7 |
| Double vessel [n (%)] | 344 (35.2) | 63 (36.8) | 3.5 |
| Triple vessel [n (%)] | 398 (40.7) | 77 (45.0) | 8.8 |
| Left main disease [n (%)] | 69 (7.1) | 15 (8.8) | 6.4 |
| Lesion type | |||
| De novo [n (%)] | 1334 (98.4) | 252 (95.8) | 15.3 |
| Intra stent [n (%)] | 17 (1.3) | 5 (1.9) | 5.2 |
| Restenosis [n (%)] | 5 (0.4) | 6 (2.3) | 16.8 |
| Lesion location | |||
| Ostial lesion [n (%)] | 160 (11.6) | 47 (17.6) | 16.9 |
| Bifurcation lesion [n (%)] | 430 (31.4) | 95 (35.4) | 8.6 |
| Number of treated lesion Median (IQR) | 1 (1-2) | 1 (1-2) | 9.9 |
| Number of stents used Median (IQR) | 2 (1-2) | 2 (1-2) | 4.8 |
| Stent type | 9.1 | ||
| Drug-eluting only [n (%)] | 1030 (99.7) | 194 (99.0) | |
| Drug-eluting and bare metal [n (%)] | 3 (0.3) | 2 (1.0) | |
| Domestic vs. imported stents | 7.0 | ||
| Domestic only [n (%)] | 544 (52.7) | 110 (56.1) | |
| Imported only [n (%)] | 462 (44.7) | 81 (41.3) | |
| Domestic and imported [n (%)] | 27 (2.6) | 5 (2.6) | |
| Intravascular ultrasound [n (%)] | 30 (2.9) | 14 (5.3) | 16.4 |
| Vascular closure devices [n (%)] | 0 (0) | 141 (71.9) | 226.4 |
"
"
| Items | TRI group | TFI group | Unadjusted OR (95%CI) | Adjusted OR (95%CI) | P value |
|---|---|---|---|---|---|
| n | 1033 | 196 | |||
| Hospital costs [mean (95%CI), CNY] | |||||
| Total cost | 59 044 (54 995-63 392) | 68 997 (63 172-75 359) | -9953 (-12 610 to -7171)* | -7495 (-10 420 to -4419)* | <0.0001 |
| PCI-related costs | 44 411 (41 604-47 407) | 50 363 (46 865-54 122) | -5952 (-7770 to -4057)* | -4067 (-6321 to -1693)* | 0.0010 |
| Hospitalization costs | 4950 (4241-5777) | 6711 (5585-8062) | -1761 (-2344 to -1100)* | -1394 (-2030 to -667)* | 0.0004 |
| Medication costs | 4653 (4273-5067) | 6080 (5015-7372) | -1427 (-2015 to -754)* | -1360 (-2003 to 614)* | 0.0007 |
| Examination costs | 5028 (4496-5622) | 5833 (5144-6615) | -806 (-1243, -327)* | -671 (-1146 to -147)* | 0.0133 |
| Clinical outcomes [n (%)] | |||||
| MACE | 30 (2.9) | 11 (5.6) | 0.50 (0.35-0.73) | 0.47 (0.31-0.73) | <0.001 |
| BARC ≥2 bleeding | 80 (7.7) | 17 (8.7) | 0.88 (0.59-1.33) | 0.98 (0.64-1.52) | 0.940 |
| BARC ≥3 bleeding | 12 (1.2) | 6 (3.1) | 0.37 (0.13-1.06) | 0.34 (0.12-1.01) | 0.051 |
| Length of stay [mean (95%CI), d] | 6.7 (6.2-7.3) | 8.9 (7.6, 10.4) | -2.2 (-2.8 to -1.4)* | -1.9 (-2.7 to -1.1)* | <0.0001 |
| Post-procedural stay [mean (95%CI), d] | 3.6 (3.2-4.1) | 4.2 (3.4, 5.1) | -0.6 (-1.0 to -0.1)* | -0.7 (-1.1 to -0.3)* | 0.0017 |
"
| Items | TRI group | TFI group | Unadjusted OR (95%CI) | Adjusted OR (95%CI) | P value |
|---|---|---|---|---|---|
| Acute myocardial infarction | |||||
| n | 176 | 23 | |||
| Total hospital costs [mean (95%CI), CNY] | 64 002 (57 669-71 031) | 79 265 (66 717-94 173) | -15 263 (-27 826, 368)* | -9812 (-21 200, 4020)* | 0.153 |
| MACE [n (%)] | 6 (3.4) | 1 (4.3) | 0.78 (0.32, 1.86) | 0.66 (0.26, 1.71) | 0.396 |
| BARC ≥2 bleeding [n (%)] | 19 (10.8) | 3 (13.0) | 0.81 (0.31, 2.10) | 1.51 (0.51, 4.51) | 0.460 |
| BARC ≥3 bleeding [n (%)] | 4 (2.3) | 1 (4.3) | 0.51 (0.12, 2.23) | 0.42 (0.09, 2.06) | 0.284 |
| Length of stay [mean (95%CI), d] | 9.2 (8.2-10.3) | 11.2 (9.2-13.6) | -2.0 (-4.0, 0.5)* | -1.0 (-3.6, 2.5)* | 0.525 |
| Postprocedural stay [mean (95%CI), d] | 4.9 (4.1-6.0) | 6.2 (4.8-8.0) | -1.3 (-2.7, 0.7)* | -0.7 (-2.2, 1.4)* | 0.462 |
| Acute coronary syndrome | |||||
| n | 730 | 133 | |||
| Total hospital costs [mean (95%CI), CNY] | 58 225 (54 095-62 671) | 71 725 (66 068-77 866) | -13 500 (-17 101, -9661)* | -12,508 (-17,524, -7023)* | <0.001 |
| MACE [n (%)] | 20 (2.7) | 8 (6.0) | 0.44 (0.26, 0.74) | 0.41 (0.25, 0.68) | <0.001 |
| BARC ≥2 bleeding [n (%)] | 60 (8.2) | 12 (9.0) | 0.90 (0.57, 1.44) | 1.12 (0.68, 1.85) | 0.657 |
| BARC ≥3 bleeding [n (%)] | 10 (1.4) | 5 (3.8) | 0.36 (0.15, 0.82) | 0.30 (0.13, 0.74) | 0.008 |
| Length of stay [mean (95%CI), d] | 6.9 (6.4-7.5) | 9.4 (8.1-10.9) | -2.3 (-3.2, -1.7)* | -2.6 (-3.5, -1.5)* | <0.001 |
| Post procedural stay [mean (95%CI), d] | 3.7 (3.2-4.1) | 4.4 (3.7-5.3) | -0.8 (-1.2, -0.2)* | -1.0 (-1.5, -0.4)* | 0.001 |
| Stable angina | |||||
| n | 274 | 56 | |||
| Total hospital costs [ mean (95%CI), CNY] | 61 039 (56 774-65 624) | 63 460 (55 034-73 177) | -2422 (-8381, 4183)* | 3710 (-2818, 11 009)* | 0.277 |
| MACE [n (%)] | 10 (3.6) | 3 (5.4) | 0.67 (0.27, 1.69) | 0.68 (0.24, 1.90) | 0.462 |
| BARC ≥2 bleeding [n (%)] | 18 (6.6) | 5 (8.9) | 0.72 (0.28, 1.86) | 0.66 (0.18, 2.41) | 0.533 |
| BARC ≥3 bleeding [n (%)] | 2 (0.7) | 1 (1.8) | 0.40 (0.04, 3.95) | 0.73 (0.07, 7.56) | 0.791 |
| Length of stay [mean (95%CI), d] | 6.1 (5.5-6.7) | 8.1 (6.8-9.6) | -2.0 (-2.7, -1.2)* | -0.7 (-1.5, -0.2)* | 0.133 |
| Post-procedural stay [mean (95%CI), d] | 3.5 (2.9-4.1) | 3.8 (3.0-4.7) | -0.3 (-0.7, 0.1)* | -0.2 (-0.5, 0.2)* | 0.430 |
| 1. | Jolly SS, Yusuf S, Cairns J, Niemelä K, Xavier D, Widimsky P, et al.Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): a randomised, parallel group, multicentre trial. Lancet 2011; 377(9775):1409-20. doi: 10.1016/S0140-6736(11)60404-2. |
| 2. | Yang Y-J, Kandzari DE, Gao Z, Xu B, Chen J-L, Qiao S-B, et al.Transradial versus transfemoral method of percutaneous coronary revascularization for unprotected left main coronary artery disease: comparison of procedural and late-term outcomes. JACC Cardiovasc Interv 2010; 3(10):1035-42. doi: 10.1016/j.jcin.2010.09.003. |
| 3. | Brueck M, Bandorski D, Kramer W, Wieczorek M, Höltgen R, Tillmanns H.A randomized comparison of transradial versus transfemoral approach for coronary angiography and angioplasty. JACC Cardiovasc Interv 2009; 2(11): 1047-54. doi: 10.1016/j.jcin.2009.07.016. |
| 4. | Feldman DN, Swaminathan RV, Kaltenbach LA, Baklanov DV, Kim LK, Wong SC, et al.Adoption of radial access and comparison of outcomes to femoral access in percutaneous coronary intervention an updated report from the National Cardiovascular Data Registry (2007-2012). Circulation 2013; 127(23):2295-306. doi: 10.1161/CIRCULATIONAHA. 112.000536. |
| 5. | Chase AJ, Fretz EB, Warburton WP, Klinke WP, Carere RG, Pi D, et al.Association of the arterial access site at angioplasty with transfusion and mortality: the MORTAL study (Mortality benefit of reduced transfusion after percutaneous coronary intervention via the arm or leg). Heart 2008; 94(8):1019-25. doi: 10.1136/hrt.2007.136390. |
| 6. | Baklanov DV, Kaltenbach LA, Marso SP, Subherwal SS, Feldman DN, Garratt KN, et al.The prevalence and outcomes of transradial percutaneous coronary intervention for ST-segment elevation myocardial infarction: analysis from the National Cardiovascular Data Registry (2007 to 2011). J Am Coll Cardiol 2013; 61(4):420-6. doi: 10.1016/j.jacc.2012.10.032. |
| 7. | Rao SV, Cohen MG, Kandzari DE, Bertrand OF, Gilchrist IC.The transradial approach to percutaneous coronary intervention: historical perspective, current concepts, and future directions. J Am Coll Cardiol 2010; 55(20):2187-95. doi: 10.1016/j.jacc.2010.01.039. |
| 8. | Romagnoli E, Biondi-Zoccai G, Sciahbasi A, Politi L, Rigattieri S, Pendenza G, et al.Radial versus femoral randomized investigation in ST-segment elevation acute coronary syndrome: the RIFLE-STEACS (Radial Versus Femoral Randomized Investigation in ST-Elevation Acute Coronary Syndrome) study. J Am Coll Cardiol 2012; 60(24):2481-9. doi: 10.1016/j.jacc.2012.06.017. |
| 9. | Jin C, Li W, Qiao SB, Yang JG, Wang Y, He PY, et al.Costs and benefits associated with transradial versus transfemoral percutaneous coronary intervention in China. J Am Heart Assoc 2016; 5(4):e002684. doi: 10.1161/JAHA.115. 002684. |
| 10. | Arnold SV, Alexander KP, Masoudi FA, Ho PM, Xiao L, Spertus JA.The effect of age on functional and mortality outcomes after acute myocardial infarction. J Am Geriatr Soc 2009; 57(2):209-17. doi: 10.1111/j.1532-5415.2008.02106.x. |
| 11. | Feldman DN, Gade CL, Slotwiner AJ, Parikh M, Bergman G, Wong SC, et al.Comparison of outcomes of percutaneous coronary interventions in patients of three age groups (< 60, 60 to 80, and> 80 years) (from the New York State Angioplasty Registry). Am J Cardiol 2006; 98(10):1334-9. doi: 10.1016/j.amjcard.2006.06.026. |
| 12. | Piper WD, Malenka DJ, Ryan TJ, Shubrooks SJ, T O’Connor G, Robb JF, et al. Predicting vascular complications in percutaneous coronary interventions. Am Heart J 2003; 145(6):1022-9. doi: 10.1016/S0002-8703(03)00079-6. |
| 13. | Assali AR, Moustapha A, Sdringola S, Salloum J, Awadalla H, Saikia S, et al.The dilemma of success: percutaneous coronary interventions in patients ≥ 75 years of age—successful but associated with higher vascular complications and cardiac mortality. Catheter Cardiovasc Interv 2003; 59(2):195-9. doi: 10.1002/ccd.10532. |
| 14. | Koutouzis M, Matejka G, Olivecrona G, Grip L, Albertsson P. Radial vs. femoral approach for primary percutaneous coronary intervention in octogenarians. Cardiovasc Revasc Med 2010; 11(2):79-83. doi: 10.1016/j.carrev.2009. 04.107. |
| 15. | Achenbach S, Ropers D, Kallert L, Turan N, Krähner R, Wolf T, et al.Transradial versus transfemoral approach for coronary angiography and intervention in patients above 75 years of age. Catheter Cardiovasc Interv 2008; 72(5): 629-35. doi: 10.1002/ccd.21696. |
| 16. | Jaffe R, Hong T, Sharieff W, Chisholm RJ, Kutryk MJB, Charron T, et al.Comparison of radial versus femoral approach for percutaneous coronary interventions in octogenarians. Catheter Cardiovasc Interv 2007; 69(6):815-20. doi: 10.1002/ccd.21021. |
| 17. | Yan ZX, Zhou YJ, Zhao YX, Liu YY, Shi DM, Guo YH, et al.Safety and feasibility of transradial approach for primary percutaneous coronary intervention in elderly patients with acute myocardial infarction. Chin Med J (Engl) 2008; 121(9):782-6. |
| 18. | He PY, Yang YJ, Qiao SB, Xu B, Yao M, Wu YJ, et al.A comparison of transradial and transfemoral approaches for percutaneous coronary intervention in elderly patients based on a propensity score analysis. Angiology 2014; 66(5):448-55. doi: 10.1177/0003319714535971. |
| 19. | Mehran R, Rao SV, Bhatt DL, Gibson CM, Caixeta A, Eikelboom J, et al.Standardized bleeding definitions for cardiovascular clinical trials a consensus report from the bleeding academic research consortium. Circulation 2011; 123(23):2736-47. doi: 10.1161/CIRCULATIONAHA.110. 009449. |
| 20. | Flury BK, Riedwyl H.Standard distance in univariate and multivariate analysis. Am Stat 1986; 40(3):249-51. |
| 21. | Austin PC.Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med 2009; 28(25):3083-107. doi: 10.1002/sim.3697. |
| 22. | Curtis LH, Hammill BG, Eisenstein EL, Kramer JM, Anstrom KJ.Using inverse probability-weighted estimators in comparative effectiveness analyses with observational databases. Med Care 2007; 45(10):S103-7. doi: 10.1097/ MLR.0b013e31806518ac. |
| 23. | Austin PC.Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm Stat 2011; 10(2):150-61. doi: 10.1002/pst.433. |
| 24. | Windecker S, Kolh P, Alfonso F, Collet J-P, Cremer J, Falk V, et al.2014 ESC/EACTS Guidelines on myocardial revascularization: the Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J 2014; 35(37):2541-619. doi: 10.1093/ eurheartj/ehu278. |
| 25. | Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, et al.2015 ACC/AHA/SCAI focused update on primary percutaneous coronary intervention for patients with ST-elevation myocardial infarction: an update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention and the 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation 2016; 133(11):1135-47. doi: 10.1161/CIR.0000000000000336. |
| 26. | Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, et al.2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol 2011; 58(24):e44-122. doi: 10.1016/j. jacc.2011.08.007. |
| 27. | Mehta RH, Rathore SS, Radford MJ, Wang Y, Wang Y, Krumholz HM.Acute myocardial infarction in the elderly: differences by age. J Am Coll Cardiol 2001; 38(3):736-41. |
| 28. | Klein LW, Block P, Brindis RG, McKay CR, McCallister BD, Wolk M, et al. Percutaneous coronary interventions in octogenarians in the American College of Cardiology-National Cardiovascular Data Registry: development of a nomogram predictive of in-hospital mortality. J Am Coll Cardiol 2002; 40(3):394-402. |
| 29. | Doyle BJ, Rihal CS, Gastineau DA, Holmes DR.Bleeding, blood transfusion, and increased mortality after percutaneous coronary intervention: implications for contemporary practice. J Am Coll Cardiol 2009; 53(22):2019-27. doi: 10.1016/j.jacc.2008.12.073. |
| 30. | Dauerman HL, Rao SV, Resnic FS,Applegate RJ.Bleeding avoidance strategies: consensus and controversy. J Am Coll Cardiol 2011; 58(1):1-10. doi: 10.1016/j.jacc.2011. 02.039. |
| 31. | Jin C, Xu Y, Qiao SB, Tang XR, Wu YJ, Yan HB, et al. Comparison of transradial and transfemoral approaches in women undergoing percutaneous coronary intervention in China: a retrospective observational study. Angiology 2017 Jan 1:3319716685670. doi: 10.1177/0003319716685670. |
| [1] | 李刚, 邴运韬, 田茂霖, 原春辉, 修典荣. 使用列线图预测老年胰腺神经内分泌肿瘤患者手术前远处转移的风险[J]. Chinese Medical Sciences Journal, 2021, 36(3): 218-224. |
| [2] | 陈强, 张丽伟, 黄党生, 张春红, 王秋霜, 沈东, 熊敏俊, 杨菲菲. 冠状动脉疾病合并糖尿病患者经StentBoost技术指导的经皮冠状动脉介入治疗后5年的随访分析[J]. Chinese Medical Sciences Journal, 2019, 34(3): 177-183. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||
|