Chinese Medical Sciences Journal ›› 2022, Vol. 37 ›› Issue (4): 309-319.doi: 10.24920/004060
Previous Articles Next Articles
Associations of Infarct Size and Regional Myocardial Function Examined by Cardiac Magnetic Resonance Feature Tracking Strain Analysis with the Infarct Location in Patients with Acute ST-Segment Elevation Myocardial Infarction
Jianing Cui, Yanan Zhao, Wei Wang, Tao Li*( )
)
- Department of Radiology, The First Medical Center, Chinese People’s Liberation Army General Hospital, Beijing 100853, China
-
Received:2022-01-14Accepted:2022-04-19Published:2022-12-31Online:2022-05-30 -
Contact:Tao Li E-mail:litaofeivip@163.com
Cite this article
Jianing Cui, Yanan Zhao, Wei Wang, Tao Li. Associations of Infarct Size and Regional Myocardial Function Examined by Cardiac Magnetic Resonance Feature Tracking Strain Analysis with the Infarct Location in Patients with Acute ST-Segment Elevation Myocardial Infarction[J].Chinese Medical Sciences Journal, 2022, 37(4): 309-319.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
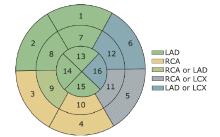
Figure 1.
Corresponding segments of left ventricular myocardium with LAD, LCX and RCA perfusion areas defined based on a myocardial 16-segment model recommendated by the American Heart Association (AHA). LAD: left anterior descending artery; LCX: left circumflex artery; RCA: right coronary artery."
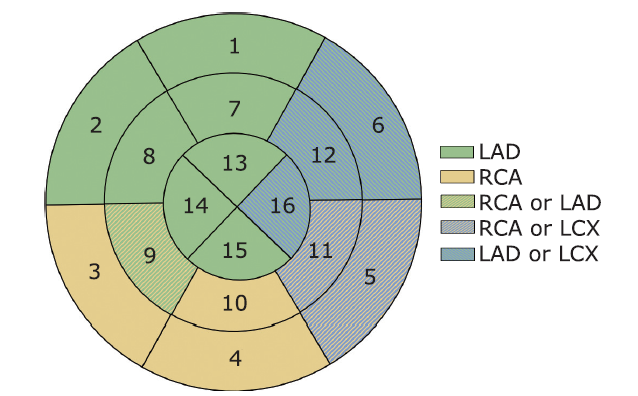
Figure 1.
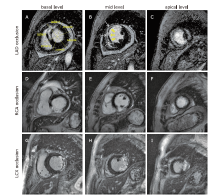
Figure 2.
Short axis late gadolinium enhancement images corresponding to LAD, RCA and LCX territories. (A-C) Representative case of anterior wall myocardial infarction [Fig. A showing infarct and remote myocardium, Fig. B showing infarct myocardium (white arrows) with microvascular obstruction (yellow arrow heads)]. (D-F) Representative case of inferior wall myocardial infarction. (G-I) Representative case of lateral wall myocardial infarction."
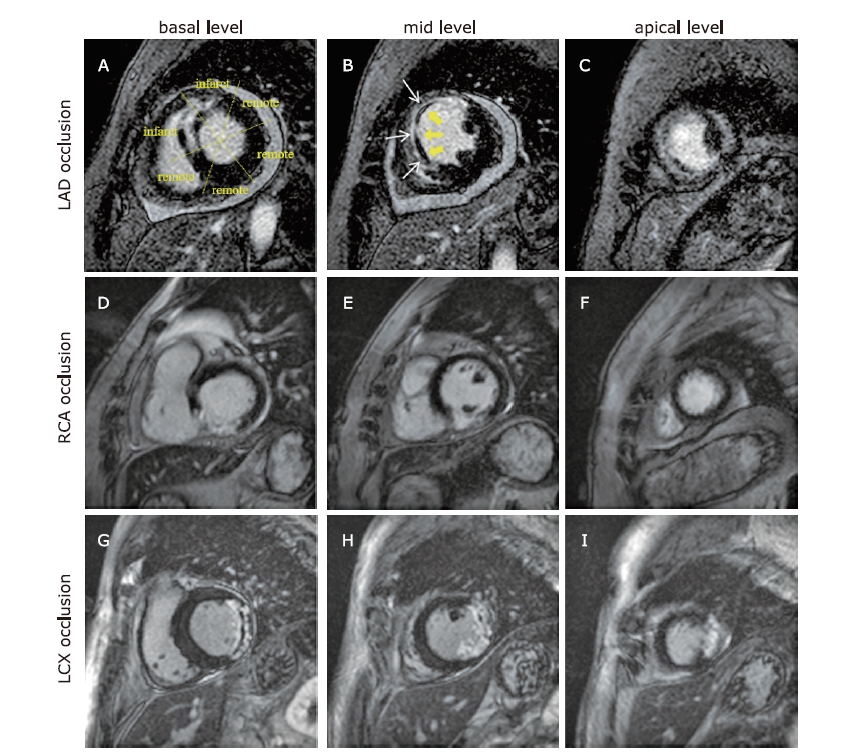
Figure 2.
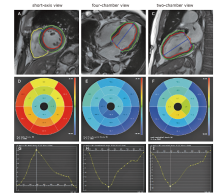
Figure 3.
Example of strain analysis in a patient with accute myocardial infaraction. (A-C) Delineations of the endocardium and epicardium on diastole phase. (D-F) Bull’s eye maps for radial, circumferential, and longitudinal strain assessments, respectively. (G-I) Strain-time graphs for radial, circumferential, and longitudinal strain assessments, respectively."
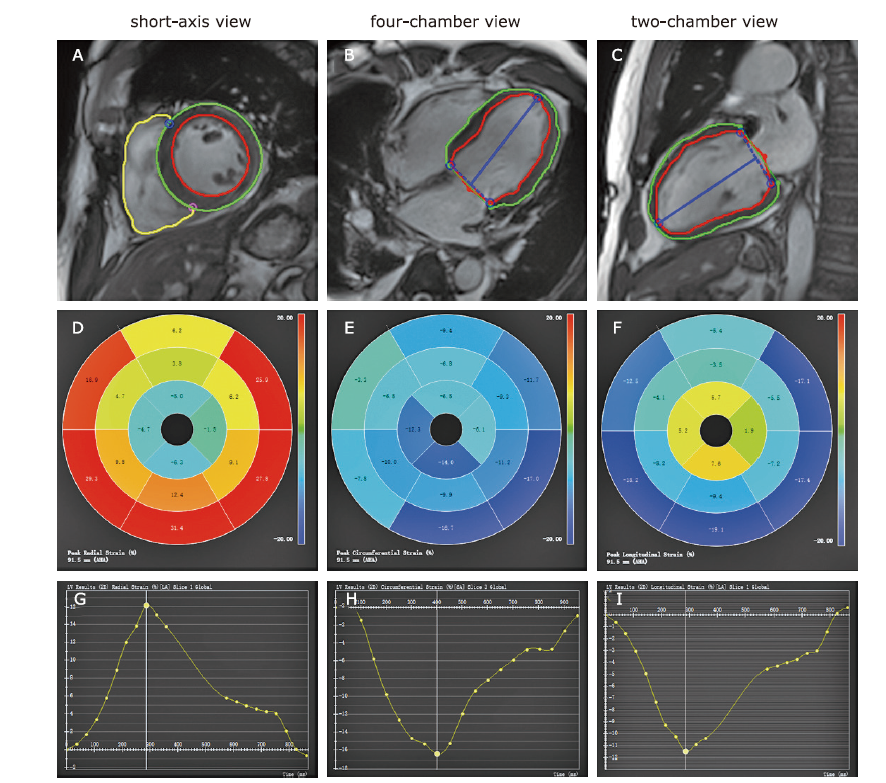
Figure 3.
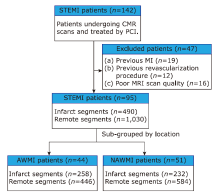
Figure 4.
Flowchart of patient enrollment. STEMI: ST-segment elevation myocardial infarction; CMR: cardiac magnetic resonance; PCI: percutaneous coronary intervention; MI: myocardial infarction; MRI: magnetic resonance imaging; AWMI: anterior wall myocardial infarction; NAWMI: nonanterior wall myocardial infarction."

Figure 4.
Table 1.
Baseline clinical characteristics of the patients with STEMI (n = 95)"
| Characteristic | Results |
|---|---|
| Age (yrs, mean ± SD) | 54.73 ± 10.74 |
| Sex [male, n (%)] | 83 (87.4) |
| Height [cm, median (IQR)] | 170 (168, 175) |
| Weight [kg, median (IQR)] | 76 (70, 85) |
| Body mass index (kg/m2, mean ± SD) | 1.91 ± 0.18 |
| Risk factors [n (%)] | |
| Smoking | 70 (73.7) |
| Family history of CAD | 9 (9.5) |
| Hypertension | 54 (56.8) |
| Diabetes mellitus | 17 (17.9) |
| Hypercholesterolemia | 28 (29.5) |
| Time interval CMR after PCI [d, mean ± SD] | 5.90 ± 2.75 |
| No. of vessels diseased [n (%)] | |
| 1 | 28 (29.5) |
| 2 | 38 (40.0) |
| 3 | 29 (30.5) |
| Infarct related artery [n (%)] | |
| LAD | 44 (46.3) |
| LCX | 9 (9.5) |
| RCA | 42 (44.2) |
Table 1.
Table 2.
CMR parameters of LV function and infarct characteristics in patients with STEMI stratified by infarct location"
| Items | AWMI (n = 44) | NAWMI (n = 51) | t/Z | P value |
|---|---|---|---|---|
| EDVI [ml/m2, median (IQR)] | 69.13 (62.25, 86.76) | 74.96 (61.61, 87.96) | -0.735 | 0.462 |
| ESVI [ml/m2, median (IQR)] | 37.44 (31.41, 50.64) | 35.28 (29.38, 46.64) | -0.623 | 0.533 |
| SVI [ml/m2, median (IQR)] | 35.86 (27.16, 43.12) | 41.33 (31.47, 46.60) | -1.638 | 0.101 |
| EF [%, median (IQR)] | 47.31 (41.17, 52.44) | 51.99 (37.48, 55.57) | -1.317 | 0.188 |
| CO [L/min, median (IQR)] | 5.02 (4.44, 5.90) | 5.29 (4.73, 6.37) | -1.482 | 0.138 |
| CI [L/min·m2, median (IQR)] | 2.72 (2.37, 3.30) | 2.77 (2.52, 3.40) | -1.015 | 0.310 |
| HR [beat/min, median (IQR)] | 71.10 (62.45, 80.95) | 65.50 (58.00, 75.40) | -1.549 | 0.121 |
| Myocardial volume [ml, median (IQR)] | 94.10 (15.50, 123.60) | 92.98 (75.27, 121.40) | -0.037 | 0.970 |
| Myocardial mass [g, median (IQR)] | 113.82 (26.88, 134.76) | 96.22 (19.12, 127.90) | -0.761 | 0.446 |
| Extent of enhanced mass (%LV, mean ± SD) | 27.47 ± 11.89 | 21.06 ± 12.08 | 3.928 | 0.008 |
| Total enhanced volume [ml, median (IQR)] | 25.37 (12.98, 38.33) | 15.25 (8.27, 27.92) | -1.918 | 0.055 |
| Total enhanced mass (g, mean ± SD) | 30.46 ± 18.11 | 24.07 ± 16.58 | 3.784 | 0.056 |
| MVO volume [ml, median (IQR)] | 2.48 (1.55, 5.35) | 1.72 (0.92, 3.98) | -1.614 | 0.106 |
| MVO mass [g, median (IQR)] | 2.80 (1.62, 5.38) | 1.81 (0.96, 4.18) | -1.560 | 0.119 |
Table 2.
Figure 5
Distribution of AWMI and NAWMI patients in the four groups of different extent of LV enhanced mass. The patients of AWMI and NAWMI were more frequently distributed in the high and low quartiles groups, respectively. The number of patients with AWMI increased with the degree of LV mass enhancement (χ2=8.941, P = 0.03)."

Figure 5
Table 3.
CMR strain characteristics of the LV myocardium in 95 STEMI patients (1,520 segments)"
| Groups | No. of segments | Peak strain [median (IQR)] | Peak systolic strain rate [median (IQR)] | Peak diastolic strain rate [median (IQR)] | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Radial (%) | Circumferential (%) | Longitudinal (%) | Radial (%/s) | Circumferential(%/s) | Longitudinal (%/s) | Radial (%/s) | Circumferential (%/s) | Longitudinal (%/s) | ||||
| Infarct segment | 490 | 12.96 (8.30, 18.95) | -9.97 (-13.26, -6.36) | -9.04 (-14.71, -4.01) | 0.83 (0.47, 1.27) | -0.69 (-0.96, -0.37) | -0.79 (-1.29, 0.62) | -0.88 (-1.33, 0.29) | 0.64 (-0.26, 0.93) | 0.78 (-0.33, 1.16) | ||
| Remote segment | 1,030 | 28.45 (19.57, 38.09) | -17.48 (-21.01, -13.54) | -13.99 (-18.55, -8.95) | 1.72 (1.22, 2.29) | -1.08 (-1.32, -0.85) | -1.13 (-1.54, -0.73) | -1.68 (-2.52, -1.09) | 1.00 (0.75, 1.29) | 0.96 (0.61, 1.36) | ||
| t/Z value | -20.873 | -20.918 | -10.357 | -19.067 | -16.586 | -7.825 | -16.731 | -15.100 | -5.454 | |||
| P value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |||
Table 3.
Table 4.
Global and infarct zone myocardial strains of the AWMI and NAWMI patient group"
| Groups | n | Peak strain [median (IQR)] | Peak systolic strain rate [median (IQR)] | Peak diastolic strain rate [median (IQR)] | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Radial (%) | Circumferential (%) | Longitudinal (%) | Radial (%/s) | Circumferential(%/s) | Longitudinal (%/s) | Radial (%/s) | Circumferential (%/s) | Longitudinal (%/s) | |||||
| Global | AWMI | 44 patients | 18.78 (15.97, 22.32) | -12.80±3.47* | -9.87 (-12.02, -8.20) | 0.98 (0.89,1.30) | -0.72 (-0.83,-0.62) | -0.60 (-0.70, -0.49) | -0.94 (-1.18,-0.64) | 0.65 (0.50,0.75) | 0.53 (0.45, 0.67) | ||
| NAWMI | 51 patients | 22.84 (18.17,26.63) | -14.36±3.14* | -12.50 (-13.45, -10.56) | 1.16 (0.89,1.48) | -0.78 (-0.88,-0.62) | -0.72 (-0.82, -0.61) | -0.98 (-1.40,-0.77) | 0.64 (0.54,0.82) | 0.62 (0.52, 0.76) | |||
| t/Z value | -2.575 | 0.001 | -4.146 | -1.280 | -0.702 | -3.181 | -1.709 | -1.112 | -2.580 | ||||
| P value | 0.010 | 0.025 | <0.001 | 0.200 | 0.483 | 0.001 | 0.087 | 0.266 | 0.010 | ||||
| Infarct zone | AWMI | 258 segments | 12.49 (7.32,18.03) | -9.54 (-12.70,-5.72) | -6.95 (-12.10,3.22) | 0.81 (0.34,1.21) | -0.67 (-0.98,0.27) | -0.62 (-1.13,0.63) | -0.81 (-1.26,0.58) | 0.64 (-0.50,0.91) | 0.63 (-0.51,0.97) | ||
| NAWMI | 232 segments | 13.82 (8.77,20.63) | -10.24 (-14.00, -7.17) | -11.68 (-16.10, -6.54) | 0.89 (0.53,1.30) | -0.71 (-0.93,-0.43) | -0.98 (-1.44,0.53) | -0.93 (-1.47,-0.47) | 0.64 (0.38,0.97) | 0.95 (0.51,1.31) | |||
| t/Z value | -2.139 | -2.086 | -6.785 | -1.909 | -1.038 | -3.634 | -2.606 | -1.824 | -4.950 | ||||
| P value | 0.032 | 0.037 | <0.001 | 0.056 | 0.299 | <0.001 | 0.009 | 0.068 | <0.001 | ||||
Table 4.

Figure 6.
Correlations between the volume and infarct characteristics of the LV with infarct zone strain. Correlation of peak systolic radial strain rate with ESVI (A) and total enhanced mass (B) in the AWMI group; Correlation of peak systolic radial strain rate with myocardial mass in the NAWMI group (C)."

Figure 6.

Figure 7.
Kaplan-Meier plot assessing event-free survival in the AWMI and NAWMI groups. The inter-observer variability of peak strain A total of 15 randomly selected patients underwent an interobserver variability analysis conducted by two independent observers. The variability assessments of peak global and infarct zone strains were shown in Table 5. Good inter-observer agreement of peak global strains (ICC 0.829, 0.859, and 0.780, respectively) and peak infarct zone strains (ICC 0.876, 0.870, and 0.899, respectively) were found."

Figure 7.
Table 5.
The inter-observer variability of peak strain"
| Items | ICC | 95%CI |
|---|---|---|
| Global | ||
| Radial | 0.829 | 0.560-0.939 |
| Circumferential | 0.859 | 0.629-0.951 |
| Longitudinal | 0.780 | 0.475-0.920 |
| Infarct zone | ||
| Radial | 0.876 | 0.678-0.956 |
| Circumferential | 0.870 | 0.666-0.954 |
| Longitudinal | 0.899 | 0.728-0.965 |
Table 5.
| [1] |
Reisinger E, Fuerstenberg T, Malyar NM, et al. German nationwide data on current trends and management of acute myocardial infarction: discrepancies between trials and real-life. Eur Heart J 2014; 35(15):979-8. doi: 10.1093/eurheartj/ehu043.
doi: 10.1093/eurheartj/ehu043 pmid: 24558113 |
| [2] |
Offi M, Patrono C, Collet JP, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J 2016; 37(3):267-15. doi: 10.1093/eurheartj/ehv320.
doi: 10.1093/eurheartj/ehv320 pmid: 26320110 |
| [3] |
O’Gara PT, Kushner FG, Ascheim DD, et al. 2013ACCF/AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2013; 127(4):529-5. doi: 10.1016/j.jacc.2012.11.018.
doi: 10.1016/j.jacc.2012.11.018 |
| [4] |
Stone PH, Raabe DS, Jaffe AS, et al. Prognostic significance of location and type of myocardial infarction: independent adverse outcome associated with anterior location. J Am Coll Cardiol 1988; 11(3):453-63. doi: 10.1016/0735-1097(88)91517-3.
doi: 10.1016/0735-1097(88)91517-3 pmid: 3278032 |
| [5] |
De Luca G, Suryapranata H, van ‘t Hof AW, et al. Prognostic assessment of patients with acute myocardial infarction treated with primary angioplasty: implications for early discharge. Circulation 2004; 109(22):2737-43. doi: 10.1161/01.CIR.0000131765.73959.87.
doi: 10.1161/01.CIR.0000131765.73959.87 pmid: 15159293 |
| [6] |
Amin ST, Morrow DA, Braunwald E, et al. Dynamic TIMI risk score for STEMI. J Am Heart Assoc 2013; 2(1):e003269. doi: 10.1161/JAHA.112.003269.
doi: 10.1161/JAHA.112.003269 |
| [7] |
Emrich T, Halfmann M, Schoepf UJ, et al. CMR for myocardial characterization in ischemic heart disease: state-of-the-art and future developments. Eur Radiol Exp 2021; 5(1):14. doi: 10.1186/s41747-021-00208-2.
doi: 10.1186/s41747-021-00208-2 pmid: 33763757 |
| [8] |
Backhaus SJ, Kowallick JT, Stiermaier T, et al. Culprit vessel-related myocardial mechanics and prognostic implications following acute myocardial infarction. Clin Res Cardiol 2020; 109(3):339-49. doi: 10.1007/s00392-019-01514-x.
doi: 10.1007/s00392-019-01514-x pmid: 31278521 |
| [9] |
Smiseth OA, T orp H, Opdahl A, et al. Myocardial strain imaging: how useful is it in clinical decision making? Eur Heart J 2016; 37(15):1196-207. doi: 10.1093/eurheartj/ehv529.
doi: 10.1093/eurheartj/ehv529 pmid: 26508168 |
| [10] |
Schuster A, Hor KN, Kowallick JT, et al. Cardiovascular magnetic resonance myocardial feature tracking: concepts and clinical applications. Circ Cardiovasc Imaging 2016; 9(4):e004077. doi: 10.1161/CIRCIMAGING.115.004077.
doi: 10.1161/CIRCIMAGING.115.004077 |
| [11] |
Shetye A, Nazir SA, Squire IB, et al. Global myocardial strain assessment by different imaging modalities to predict outcomes after ST-elevation myocardial infarction: a systematic review. World J Cardiol 2015; 7(12):948-60. doi: 10.4330/wjc.v7.i12.948.
doi: 10.4330/wjc.v7.i12.948 pmid: 26730301 |
| [12] |
Kirkpatrick JN, Vannan MA, Narula J, et al. Echocardiography in heart failure: applications, utility, and new horizons. J Am Coll Cardiol 2007; 50(5):381-96. doi: 10.1016/j.jacc.2007.03.048.
doi: 10.1016/j.jacc.2007.03.048 pmid: 17662389 |
| [13] |
Bodi V. Strain by feature tracking: a short summary of the journey of CMR in STEMI. JACC Cardiovasc Imaging 2019; 12(7 Pt 1):1199-201. doi: 10.1016/j.jcmg.2018.08.009.
doi: 10.1016/j.jcmg.2018.08.009 |
| [14] |
Zghal FM, Boudiche S, Haboubi S, et al. Diagnostic accuracy of strain imaging in predicting myocardial viability after an ST-elevation myocardial infarction. Medicine (Baltimore) 2020; 99(19): e19528. doi: 10.1097/MD.0000000000019528.
doi: 10.1097/MD.0000000000019528 |
| [15] |
Eitel I, Stiermaier T, Lange T, et al. Cardiac magnetic resonance myocardial feature tracking for optimized prediction of cardiovascular events following myocardial infarction. JACC Cardiovasc Imaging 2018; 11(10):1433-44. doi: 10.1016/j.jcmg.2017.11.034.
doi: S1936-878X(17)31176-2 pmid: 29454776 |
| [16] |
Valente F, Gutierrez L, Rodríguez-Eyras L, et al. Cardiac magnetic resonance longitudinal strain analysis in acute ST-segment elevation myocardial infarction: a comparison with speckle-tracking echocardiography. Int J Cardiol Heart Vasc 2020; 29:100560. doi: 10.1016/j.ijcha.2020.100560.
doi: 10.1016/j.ijcha.2020.100560 |
| [17] |
Nazir SA, Shetye AM, Khan JN, et al. Inter-study repeatability of circumferential strain and diastolic strain rate by CMR tagging, feature tracking and tissue tracking in ST-segment elevation myocardial infarction. Int J Cardiovasc Imaging 2020; 36(6):1133-46. doi: 10.1007/s10554-020-01806-8.
doi: 10.1007/s10554-020-01806-8 pmid: 32152811 |
| [18] |
Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. Eur Heart J 2012; 33(20):2551-67. doi: 10.1093/eurheartj/ehs184.
doi: 10.1093/eurheartj/ehs184 pmid: 22922414 |
| [19] |
Eite I, Desch S, Fuernau G, et al. Prognostic significance and determinants of myocardial salvage assessed by cardiovascular magnetic resonance in acute reperfused myocardial infarction. J Am Coll Cardiol 2010; 55(22):2470-9. doi: 10.1016/j.jacc.2010.01.049.
doi: 10.1016/j.jacc.2010.01.049 pmid: 20510214 |
| [20] |
Cerqueira MD, Weissman NJ, Dilsizian V, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation 2002; 105(4):539-42. doi: 10.1161/hc0402.102975.
doi: 10.1161/hc0402.102975 pmid: 11815441 |
| [21] |
Mahmarian JJ, Pratt CM, Boyce TM, et al. The variable extent of jeopardized myocardium in patients with single vessel coronary artery disease: quantification by thallium 201 single photon emission computed tomography. J Am Coll Cardiol 1991; 17(2):355-62. doi: 10.1016/s0735-1097(10)80099-3.
doi: 10.1016/s0735-1097(10)80099-3 pmid: 1991891 |
| [22] |
Lee JT, Ideker RE, Reimer KA. Myocardial infarct size and location in relation to coronary vascular bed at risk in man. Circulation 1981; 64(3):526-34. doi: 10.1161/01.cir.64.3.526.
doi: 10.1161/01.cir.64.3.526 pmid: 7261285 |
| [23] |
Elsman P, van ‘t Hof AW, de Boer MJ, et al. Impact of infarct location on left ventricular ejection fraction after correction for enzymatic infarct size in acute myocardial infarction treated with primary coronary intervention. Am Heart J 2006; 151(6): 1239.e9-14. doi: 10.1016/j.ahj.2005.12.006.
doi: 10.1016/j.ahj.2005.12.006 |
| [24] |
Reinstadler SJ, Thiele H, Eite I. Risk stratification by cardiac magnetic resonance imaging after ST -elevation myocardial infarction. Curr Opin Cardiol 2015; 30(6):681-9. doi: 10.1097/HCO.0000000000000227.
doi: 10.1097/HCO.0000000000000227 pmid: 26398412 |
| [25] |
Eite I, de Waha S, Wöhrle J, et al. Comprehensive prognosis assessment by CMR imaging after ST-segment elevation myocardial infarction. J Am Coll Cardiol 2014; 64(12):1217-26. doi: 10.1016/j.jacc.2014.06.1194.
doi: 10.1016/j.jacc.2014.06.1194 pmid: 25236513 |
| [26] |
Wu KC. CMR of microvascular obstruction and hemorrhage in myocardial infarction. J Cardiovasc Magn Reson 2012; 14(1): 68. doi: 10.1186/1532-429X-14-68.
doi: 10.1186/1532-429X-14-68 |
| [27] |
Reindl M, Holzknecht M, Tiller C, et al. Impact of infarct location and size on clinical outcome after ST-elevation myocardial infarction treated by primary percutaneous coronary intervention. Int J Cardiol 2020; 301:14-20. doi: 10.1016/j.ijcard.2019.11.123.
doi: S0167-5273(19)33043-8 pmid: 31761400 |
| [28] |
Podlesnikar T, Pizarro G, Fernández-Jiménez R, et al. Left ventricular functional recovery of infarcted and remote myocardium after ST-segment elevation myocardial infarction (METOCARD-CNIC randomized clinical trial substudy). J Cardiovasc Magn Reson 2020; 22 (1): 44. doi: 10.1186/s12968-020-00638-8.
doi: 10.1186/s12968-020-00638-8 |
| [29] |
Li S, Zhao L, Lu A, et al. Comparison of left ventricular global strain in anterior and non-anterior wall myocardial infarction with CMR tissue tracking. Front Physiol 2020; 11:530108. doi: 10.3389/fphys.2020.530108.
doi: 10.3389/fphys.2020.530108 |
| [30] |
Bogaert J, Bosmans H, Maes A, et al. Remote myocardial dysfunction after acute anterior myocardial infarction: impact of left ventricular shape on regional function: a magnetic resonance myocardial tagging study. J Am Coll Cardiol 2000; 35(6):1525-34. doi: 10.1016/s0735-1097(00)00601-x.
doi: 10.1016/s0735-1097(00)00601-x pmid: 10807456 |
| [31] |
Claus P, Omar AMS, Pedrizzetti G, et al. Tissue tracking technology for assessing cardiac mechanics: principles, normal values, and clinical applications. JACC Cardiovasc Imaging 2015; 8(12):1444-60. doi: 10.1016/j.jcmg.2015.11.001.
doi: S1936-878X(15)00845-1 pmid: 26699113 |
| [1] | Ya-Nan Zhao, Jia-Ning Cui, Xing-Hua Zhang, Jin-Feng Li, Shi-Min Chen, Xiu-Zheng Yue, Tao Li. Relationship of Microvascular Obstruction with Global and Regional Myocardial Function Determined by Cardiac Magnetic Resonance after ST-Segment Elevation Myocardial Infarction [J]. Chinese Medical Sciences Journal, 2023, 38(1): 11-19. |
| [2] | Xuewei Huang, Keqiong Deng, Juanjuan Qin, Fang Lei, Xingyuan Zhang, Wenxin Wang, Lijin Lin, Yuming Zheng, Dongai Yao, Huiming Lu, Feng Liu, Lidong Chen, Guilan Zhang, Yueping Liu, Qiongyu Yang, Jingjing Cai, Zhigang She, Hongliang Li. Association Between Lipid Profiles and Left Ventricular Hypertrophy: New Evidence from a Retrospective Study [J]. Chinese Medical Sciences Journal, 2022, 37(2): 103-117. |
| [3] | Liu Zhijian, Hu Gaopin, Fei Meiying, Yin Zao, Shi Quanxing, Sun Fei. Effects of Short-term High Dose Atorvastatin on Left Ventricular Remodeling in Patients with First Time Attack of Anterior Acute Myocardial Infarction [J]. Chinese Medical Sciences Journal, 2018, 33(2): 84-90. |
| [4] | Ying Fan, Shan-xiao Zhang, Meng Ren, Li-feng Hong, Xiao-ni Yan. Impact of 1, 25-(OH)2D3 on Left Ventricular Hypertrophy in Type 2 Diabetic Rats [J]. Chinese Medical Sciences Journal, 2015, 30(2): 114-120. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
|