

AMYOTROPHIC lateral sclerosis (ALS) is a progressive neurodegenerative disease with selected both upper and lower motor neuron lesions. [1,2] In ALS, many voxel-based morphometry (VBM) studies found that gray matter (GM) volume decreased widely, especially in motor cortex, [3,4] frontal and temporal regions, [4,5,6] corpus callosum, [7 amygdala, [8 caudate nucleus head. [9 However, Mezzapesa et al’s study showed that no volume reduction of primary motor cortices in ALS patients. [10 Voxel-wise meta-analysis[11-12 has revealed that ALS is a complex degenerative disease involving multi-systems besides motor system, and right precentral GM atrophy is a common finding and prominent feature of brain structural changes in ALS. [13] However, GM changes over the whole brain were not comprehensively studied in bulbar-onset and spinal-onset ALS patients.
The aim of this study is to investigate brain structural imaging signatures in clinical subtypes of ALS. We hypothesized that some brain regions may intrinsically suffered from volume loss in the patients with ALS. To address this hypothesis, we obtained brain structure images of 65 patients with ALS (ALS group) and 65 normal controls (NC) from 3.0T MRI system. All the ALS patients were classified into bulbar-onset group (ALS-bulbar, n=15) and spinal-onset group (ALS-spinal, n=50) according to the initial onset location. We firstly identified the alteration of GM changes over the whole brain between the ALS group and the NCs, and then the GM volume analysis was performed among the ALS-bulbar group, ALS-spinal group and the control group to identify the pattern of different GM volume loss.
PATIENTS AND METHODS
Participants
This study was approved by the institutional ethic review board and written informed consents were obtained from all participants. Sixty-five patients, including 34 cases with definite diagnosis of ALS and 31 cases with suspicious diagnosis of ALS according to the revised El Escorial, [14] were consecutively recruited from the Chinese PLA General Hospital from 2007 to 2010. The subjects were excluded for the following conditions: 1. history of cerebrovascular disease, long-standing hypertension, diabetes mellitus, inflammatory disease of the central nervous system and cranium trauma; 2. taking psychoactive drugs or hormone; 3. structural damage observed on the conventional MR images. All the subjects were right handed. ALS functional rating score (ALSFRS) [15] and Norris Scale[16] were administered to all the patients for clinical rating their ALS symptoms, and mini-mental state examination (MMSE) [17] was applied to evaluate the cognitive function of all subjects.
MRI examination and acquisition
MR structural images were obtained from a 3.0T MR imaging system (SIGNA EXCITE, GE Healthcare, Milwaukee, WI, USA) and a conventional eight-channel quadrature head coil. Three-dimensional T1-weighted fast spoiled gradient recalled echo (3D T1-FSPGR) sequence was used, and the parameters were as follows: TR (repetition time) = 6.3 ms, TE (echo time) =2.8 ms, flip angle = 15°, FOV (field of view) = 24 cm×24 cm, Matrix = 256×256, in-plane resolution of 0.9375×0.9375 mm2, NEX (number of acquisition) = 1. Conventional T2-weighted images, T1-weighted images and diffusion weighted images were also obtained to exclude the patients with diseases other than ALS that inflecting brain morphometry. The imaging protocol was identical to each subject.
Data processing
All MR structural image data were processed using Statistical Parametric Mapping 12 (SPM 12) (http://www.fil.ion.ucl.ac.uk/spm/) running under MATLAB 7.6 (The Mathworks, Natick, MA, USA) to perform VBM. [18] The preprocess of VBM was as follows: (1) setting the image origin at the anterior commissure (AC); (2) normalizing the individual structural images to the DARTEL (Diffeomorphic Anatomical Registration using Exponentiated Lie algebra) templates space; (3) segmenting the normalized images into GM, white matter and cerebrospinal fluid (CSF); (4) calculating the volume of 142 brain regions based on SPM Neuromorphometrics atlas; total GM volume (TGMV), total white matter volume (TWMV), and total CSF volume (TCSFV) were recorded. Total intracranial volume (TIV) was the sum of the volume of segmented brain tissue (TIV = TGMV + TWMV + TCSFV), and fraction of GMV (fGMV) was the ratio of TGMV to TIV (fGMV = TGMV/TIV); (5) smoothing the segmented GM images with a kernel of 8 mm FWHM (full width at half maxima) before statistical analysis.
Statistical analysis
VBM was performed using two-sample t test with TIV, age and sex as covariates by the factorial design specification tools of SPM. Significance was set if a Puncorr value<0.001. The cluster size was listed as K value, and the difference of the cluster between two groups was represented by T value. The minimal number of contiguous voxels was set based on the expected voxels per cluster.
The quantitative data with normal distribution were presented as mean ± standard deviation, and the quantitative data with nonnormal distribution were presented as median ± interquartile range. The partial correlation analysis was applied between the clinical variables (ALSFRS, disease duration, Norris score, MMSE) and volume of abnormal brain regions in ALS patients. The group difference for the abnormal brain regions was compared using ANCOVA covarying with age and sex, and the Welch test was used because of variance non-homogeneity. The statistical analysis was performed using SPSS 19.0.
RESULTS
Demography and clinical scale test
The participants came from 10 provinces and included 63 sporadic cases and 2 familial cases. There were 28 female and 37 males in the ALS group, 29 females and 36 males in the NC group (χ2=0.03, P=0.86). The age of the two group were 49.63±10.25 years old and 43.48±12.22 years old (t=1.98, P=0.002). The MMSE of the ALS patients and NCs were comparable (both 28.00±3.00, t=1.98, P=43). For ALS patients, the average of disease duration, ALSFRS and Norris scores were 17.74±21.46 months, 30.00±7.00 (normal value 48) and 69.00±28.50 (normal value 99), respectively.
GM volume changes over the whole brain of ALS patients
In patients with ALS, the decreased GM volume of brain regions, compared with NC, located in the right precentral gyrus (rPrcGy) [MNI coordinate (x, y, z): 39, -12, 53; K value: 624; T value: 4.38; P value: 0.000] and right middle frontal gyrus (rMidFroGy) [MNI coordinate (x, y, z): 42, 56, 11; K value: 150; T value: 3.88; P value: 0.000]. No increased GM volume of brain region in ALS was recognized (Fig. 1).
Figure 1.
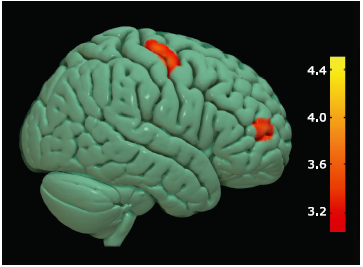
Figure 1.
Brain region with decreased gray matter (GM) volume in ALS group compared with NC group.
Colored areas represent the involved brain areas: right precentral gyrus and middle frontal gyrus respectively. The value of the color bar represents T value.
ANCOVA demonstrated the GM volume of the rPrcGy were significant different between the ALS and the NC groups (P=0.03). No significant difference of TGMV, TIV and fGMV was observed for the rMidFroGy between the ALS and NC group (all P>0.05) (Table 1).
Table 1 Volume comparisons of rPrcGy, rMidFroGy, TGMV, TIV and fGMV between the ALS and NC groups (10-3 ml, n=65)
| Groups | Volume of rPrcGy | Volume of rMidFroGy | |||||
|---|---|---|---|---|---|---|---|
| means±SD | 95% CI | means±SD | 95% CI | ||||
| NCs | 12.14±1.33 | 11.68-12.30 | 18.71±2.41 | 17.84-18.97 | |||
| ALS | 11.36±1.34 | 11.19-11.81 | 17.64±2.61 | 17.38-18.51 | |||
| F value | 4.76 | 1.26 | |||||
| P value* | 0.03 | 0.27 | |||||
| Groups | TGMV | TIV | fGMV | ||||
| means±SD | 95% CI | means±SD | 95% CI | means±SD | 95% CI | ||
| NCs | 610.75±56.74 | 589.83-617.29 | 1423.72±127.38 | 1385.11-1453.02 | 0.43±0.02 | 0.42-0.43 | |
| ALS | 574.72±64.43 | 578.18-605.64 | 1393.96±144.74 | 1364.66-1432.57 | 0.42±0.02 | 0.41-0.43 | |
| F value | 1.36 | 0.69 | 0.41 | ||||
| P value* | 0.25 | 0.41 | 0.52 | ||||
*analysis of covariance was performed for comparisons adjusted by age. NC: normal control; ALS: amyotrophic lateral sclerosis; rPreGy: right precentral gyrus; rMidFroGy: right middle frontal gyrus; TGMV: total gray matter volume; TIV: total intracranial volume; fGMV: fraction of gray matter volume (=TGMV/TIV).
GM volume changes between ALS-bulbar and NC
In patients with ALS-bulbar, compared with NCs, the decreased GM volume was located in the left medial orbital gyrus [MNI coordinate (x, y, z): -11, 41, -30; K value: 125; T value: 4.09; P value: 0.000], the left inferior temporal gyrus [MNI coordinate (x, y, z): -53, -32, -21; K value: 418; T value: 4.87; P value: 0.000]and the right middle temporal gyrus [MNI coordinate (x, y, z): 65, -32, -14; K value: 134; T value: 4.16; P value: 0.000] (Fig. 2). No increased GM volume in ALS-bulbar was recognized.
Figure 2.
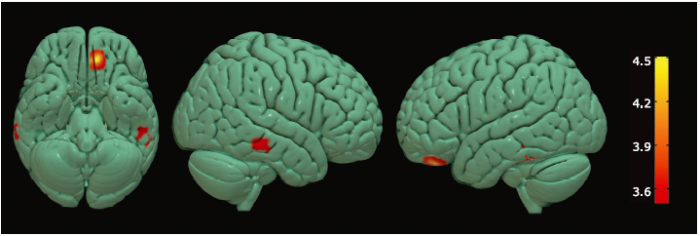
Figure 2.
Brain regions with decreased GM volume in bulbar-onset ALS patients compared with NC group.
Colored areas represent the involved brain areas, including left medial orbital gyrus, left inferior temporal gyrus and right middle temporal gyrus group respectively. The value of the color bar represents T value.
Among the above three regions with loss of GM, only the volume of the left inferior temporal gyrus in the ALS-bulbar was found to have significant difference from the NCs (F=6.19, P=0.02). The GMV, fGMV and TIV were not significantly different between the ALS-bulbar and NC groups (Table 2).
Table 2 Volume comparisons of the brain regions with decreased GMV and TGMV, TIV, fGMV between the ALS-bulbar and NC groups (10-3 ml)
| Groups | n | Volume of lMedOrbGy | Volume of lInfTemGy | Volume of rMidTemGy | |||
|---|---|---|---|---|---|---|---|
| means±SD | 95% CI | means±SD | 95% CI | means±SD | 95% CI | ||
| NCs | 65 | 4.40±0.57 | 4.08-4.64 | 10.00±1.00 | 9.39-10.59 | 14.14±1.97 | 13.09-14.76 |
| bulbar-onset ALS | 15 | 4.15±0.51 | 3.91-4.47 | 8.94±1.17 | 8.35-9.55 | 13.49±1.46 | 12.87-14.54 |
| F value | 0.70 | 6.19 | 0.14 | ||||
| P value* | 0.41 | 0.02 | 0.71 | ||||
| Groups | n | TGMV | TIV | fGMV | |||
| means±SD | 95% CI | means±SD | 95% CI | means±SD | 95% CI | ||
| NCs | 65 | 610.75±56.74 | 589.83-617.29 | 1423.72±127.38 | 1385.11-1453.02 | 0.43±0.02 | 0.42-0.43 |
| bulbar-onset ALS | 15 | 577.18±65.12 | 554.32-614.58 | 1366.53±133.84 | 1309.04-1441.14 | 0.42±0.02 | 0.41-0.44 |
| F value | 0.07 | 0 | 0.32 | ||||
| P value* | 0.80 | 0.98 | 0.58 | ||||
*Analysis of covariance was performed for the group comparisons covarying with age. lMedOrGY: left medial orbital gyrus; lInfTemGy: left inferior temporal gyrus; rMidTemGy: right middle temporal gyrus.
GM volume changes between ALS spinal and NC
Compared with the NC group, the decreased GM volume of brain regions in the ALS-spinal group were located in the rPrcGy, left medial precentral gyrus, left postcentral gyrus, bilateral superior frontal gyrus, right middle frontal gyrus, bilateral middle occipital gyrus, bilateral angular gyrus, right middle temporal gyrus, left thalamus proper (lThaPro), left central operculum, left supramarginal gyrus, left precuneus, left inferior frontal angular gyrus, left fusiform gyrus, and left superior parietal lobule (Table 3, Fig. 3) .
Figure 3.
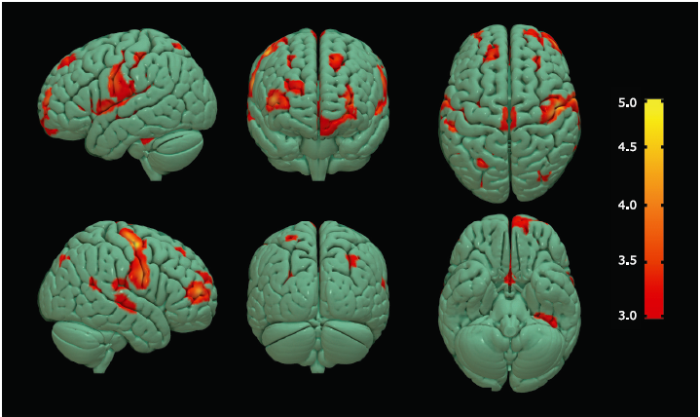
Figure 3.
Brain regions with decreased GM volume in ALS-spinal patients compared with NC group.
Multiple colored areas represent the involved brain regions, including bilateral precentral gyrus (right precentral gyrus dominance) and the other multiple brain regions. The value of the color bar represents T value.
Table 3 Brain regions with decreased GM volume in patients with ALS-spinal compared with NCs
| Anatomic region | MNI-space | K value | P value | T value | ||
|---|---|---|---|---|---|---|
| X | Y | Z | ||||
| Left Thalamus Proper | -21 | -21 | 12 | 928 | 0.000 | 5.58 |
| Right Precentral Gyrus | 48 | -9 | 57 | 2753 | 0.000 | 5.46 |
| Left Superior Frontal Gyrus | -18 | 54 | 6 | 4582 | 0.000 | 5.35 |
| Left Postcentral Gyrus | -54 | -8 | 33 | 4032 | 0.000 | 5.15 |
| Right Middle Frontal Gyrus | 42 | 53 | 9 | 1015 | 0.000 | 4.88 |
| Left Central Operculum | -54 | 2 | 3 | 633 | 0.000 | 4.27 |
| Right Superior Frontal Gyrus | 23 | 54 | 21 | 351 | 0.000 | 4.24 |
| Right Middle Occipital Gyrus | 32 | -75 | 41 | 215 | 0.000 | 4.15 |
| Left Supramarginal Gyrus | -45 | -48 | 24 | 141 | 0.000 | 4.14 |
| Left Precuneus | -5 | -65 | 27 | 1157 | 0.000 | 4.06 |
| Left Middle Occipital Gyrus | -29 | -80 | 15 | 293 | 0.000 | 4.00 |
| Left Medial Precentral Gyrus | 0 | -18 | 75 | 220 | 0.000 | 3.97 |
| Right Superior Frontal Gyrus | 26 | 33 | 47 | 123 | 0.000 | 3.96 |
| Right Middle Temporal Gyrus | 60 | -20 | -8 | 274 | 0.000 | 3.95 |
| Right Angular Gyrus | 57 | -48 | 18 | 166 | 0.000 | 3.87 |
| Left Angular Gyrus | -48 | -60 | 35 | 153 | 0.000 | 3.78 |
| Left Inferior Frontal Angular Gyrus | -48 | 26 | 6 | 130 | 0.000 | 3.74 |
| Left Fusiform Gyrus | -32 | -33 | -29 | 177 | 0.000 | 3.70 |
| Left Superior Frontal Gyrus | -17 | 39 | 48 | 300 | 0.000 | 3.69 |
| Left Superior Parietal Lobule | -26 | -54 | 56 | 176 | 0.000 | 3.67 |
MNI: Montreal Neurological Institute; X, Y, Z: coordinates of the primary maximum of the cluster. (T>3.18, Puncorr value<0.001, expected 122 voxels per cluster)
Differences of GM volume alterations between ALS-spinal and ALS-bulbar
Compared with ALS-bulbar, the ALS-spinal presented decreased GM volume in the left postcentral gyrus [MNI coordinate (x, y, z): -65, -5, 29; K value: 335; T value: 4.32; P value: 0.000]; meanwhile, the ALS-bulbar presented decreased GM volume in the left middle temporal gyrus (MNI coordinate (x, y, z): -59, -29, -18; K value: 281; T value: 4.07; P value: 0.000) compared with ALS-spinal (Fig. 4).
Figure 4.
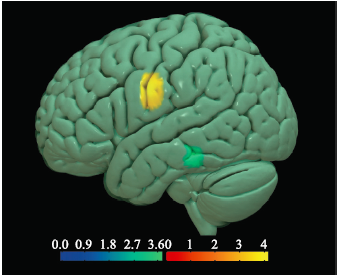
Figure 4.
Brain regions with altered volume of GM in the ALS-spinal and ALS-bulbar.
Hot cluster in yellow, located in the left postcentral gyrus, represented the decreased volume in ALS-spinal compared with ALS-bulbar; cold cluster in green, located in the left middle temporal gyrus, represented decreased volume in ALS-bulbar compared with ALS-spinal.
Correlation analysis between regional volume changes and the clinical features
In ALS patients, the volume of rPrcGy was positively correlated with ALSFRS (r=0.299, P=0.017). In ALS-bulbar patients, volume of the left medial orbital gyrus, left inferior temporal gyrus, right middle temporal gyrus was not found to correlate with any of clinical variables (disease duration, ALSFRS or Norris score). In ALS-spinal patients, there was a significant negative correlation between the volume of the lThaPro and the disease duration (r=-0.383, P=0.007), and no correlation was found between the volume of lThaPro and ALSFRS, or Norris score.
DISCUSSION
This study demonstrated that the rPreGy presented volume loss in the ALS patients. This result was consistent with the previous studies, [11,12,13] which suggested that the rPreGy atrophy may be a MRI structural signature for ALS, disregarding its clinical type. VBM analysis demonstrated that atrophy of rPreGy presented only in ALS-spinal patients, but not in ALS-bulbar patients. Therefore, VBM technique could elucidate the different nuromechanism for the different ALS subtypes, and provide a valuable method to understand the structure changes of motor cortex in ALS. The finding of rPreGy atrophy on voxel-level might be explained by the decreased number and shape of cortical neurons[19,20] from the pathological viewpoints.
Further analysis in the clinical subtypes demonstrated that bulbar-onset and spinal-onset ALS presented different patterns of GM atrophy. For the bulbar-onset ALS, only extra-motor brain regions were involved, and the motor cortex was spared. The involved brain regions were located in frontal lobe (left medial orbital gyrus) and temporal lobe (left inferior temporal gyrus and right middle temporal gyrus). These findings may be associated with the poorer cognitive function in bulbar-onset ALS patients than those of spinal-onset subtype. [21] Therefore, bulbar subtype may be considered as fronto-temporal pattern ALS, and the longitudinal observe will help to understand the association between ALS and fronto-temporal dementia.
However, the analysis of the whole brain region involvement for the bulbar-onset ALS patients showed that only left inferior temporal gyrus was significantly different from the controls. This finding suggested that the left inferior temporal gyrus was the key damaged brain region in bulbar-onset ALS patients.
In patients with spinal-onset ALS, our study demonstrated that motor and extra-motor brain regions were both involved compared with NCs. The involved motor brain regions included the rPreGy (2753 voxels) and left medial precentral gyrus (220 voxels), which was consistent with previous studies, [4, 22,23,24,25] and could underlie the pathological characteristics[26,27] and MRS findings[28] in ALS. However, some studies reported no atrophy of motor cortex, [5, 10, 29] and some study found the metabolic changes took place in motor cortex of ALS patients, with no concomitant anatomical change. [30] The reasons for the inconsistence might be associated with heterogeneity course of pathologic process and the different clinical features, such as initial onset of the ALS patients in this study. The result of this study indicated that motor cortex atrophy was the MRI signature of spinal-onset ALS.
Extra-motor GM involvement was also demonstrated in this study, which could be considered as a substantial feature of ALS. The extra-motor GM damage involved bilateral frontal cortex, right temporal cortex, as well as the other brain region where GM volume loss. Bilateral superior frontal gyrus presented significant GM loss, indicating that these brain regions may play a critical role in motor response inhibition[31] and recovery of language function[32] in ALS patients. Since left inferior frontal gyrus also plays a critical role in integrating individual word meanings to coherent sentence-level messages[33] and language production, [34] the volume loss of frontal gray matter we found in this study may help to understand the verbal fluency deficits of ALS. [35,36,37]
In this study we found that GM deficits distributed widely in the whole brain of spinal-onset ALS compared with bulbar-onset ALS. In clinical practice, the bulbar-onset ALS is less common than spinal-onset ALS; [38] however, 48% of ALS patients were identified with cognitive impairment, [39] and the abnormalities indicated fronto-temporal involvement. Our results suggest that widespread GM loss of extra-motor cortex such as frontal lobe and temporal lobe exists in spinal-onset ALS patients compared with bulbar-onset ALS patients. The extensive atrophy of extra-motor cortex also suggests that more upper motor neurons may be involved in spinal-onset ALS than bulbar-onset ALS patients. These findings may also reflect the heterogeneity of clinical onsets in ALS patients, and provide useful information to better understand the cognitive impairment in ALS.
VBM analysis demonstrated the differences existed between bulbar- and spinal-onset ALS. The volume of left postcentral gyrus in spinal-onset ALS and left middle temporal gyrus in bulbar-onset ALS were significantly different compared to each other. This finding indicates the intrinsic difference may exist between the clinical sub-types of ALS, and its clinical significance should be investigated in future.
The limits of this study included: (1) The samples presented heterogeneity, and the bulbar-onset ALS sample was relatively small; (2) Although MMSE was performed to exclude dementia, the mild cognitive impairment was not evaluated in detail.
To conclude, these findings supported that the atrophy of rPreGy might be used as a feasible imaging biomarker for diagnosis of ALS. Extra-motor GM atrophy (fronto-temporal pattern) is a MRI structural signature in bulbar-onset ALS patients. Motor and extra-motor (fronto-temporal and extra-fronto-temporal pattern) GM atrophy were structural signatures on MRI in spinal-onset ALS patients. VBM is a sensitive and effective tool for brain structure evaluation in patients with ALS.
参考文献
Upper motor neuron and extra-motor neuron involvement in amyotrophic lateral sclerosis: a clinical and brain imaging review
There is an ongoing discussion whether ALS is primarily a disease of upper motor neurons or lower motor neurons. We undertook a review to assess how new insights have contributed to solve this controversy. For this purpose we selected relevant publications from 1995 onwards focussing on (1) primary targets and disease progression in ALS and variants of ALS, (2) brain imaging markers for upper motor neuron lesion, and (3) evidence for ALS being a multisystem disorder. Clinically, upper motor and lower motor neuron symptoms can occur in any order over time. Brain imaging markers show upper motor neuron involvement in early disease. Overlap syndromes of ALS and dementia, and involvement of autonomic and sensory nerves occur frequently. PET/SPECT scans, functional MRI and voxel based morphometry studies clearly show abnormalities in extra-motor areas of the brain. Pathologically, the 43 kDa TAR DNA-binding protein (TDP-43) provides a clue to these overlapping disorders. In conclusion, evidence accumulates that ALS is a multisystem disorder rather than a pure lower and/or upper motor neuron disorder.
Voxel-based MRI intensitometry reveals extent of cerebral white matter pathology in amyotrophic lateral sclerosis
Amyotrophic lateral sclerosis (ALS) is characterized by progressive loss of upper and lower motor neurons. Advanced MRI techniques such as diffusion tensor imaging have shown great potential in capturing a common white matter pathology. However the sensitivity is variable and diffusion tensor imaging is not yet applicable to the routine clinical environment. Voxel-based morphometry (VBM) has revealed grey matter changes in ALS, but the bias-reducing algorithms inherent to traditional VBM are not optimized for the assessment of the white matter changes. We have developed a novel approach to white matter analysis, namely voxel-based intensitometry (VBI). High resolution T1-weighted MRI was acquired at 1.5 Tesla in 30 ALS patients and 37 age-matched healthy controls. VBI analysis at the group level revealed widespread white matter intensity increases in the corticospinal tracts, corpus callosum, sub-central, frontal and occipital white matter tracts and cerebellum. VBI results correlated with disease severity (ALSFRS-R) and patterns of cerebral involvement differed between bulbar- and limb-onset. VBI would be easily translatable to the routine clinical environment, and once optimized for individual analysis offers significant biomarker potential in ALS.
Neuroimaging in amyotrophic lateral sclerosis
Widespread sensorimotor and frontal cortical atrophy in Amyotrophic Lateral Sclerosis
Background Widespread cortical atrophy in Amyotrophic Lateral Sclerosis (ALS) has been described in neuropathological studies. The presence of cortical atrophy in conventional and scientific neuroimaging has been a matter of debate. In studies using computertomography, positron emission tomography, proton magnetic resonance spectroscopy and conventional T2-weighted and proton-weighted images, results have been variable. Recent morphometric studies by magnetic resonance imaging have produced conflicting results regarding the extent of grey and white matter involvement in ALS patients. Methods The authors used optimized voxel-based morphometry as an unbiased whole brain approach to detect differences between regional grey and white matter volumes. Seventeen patients with a diagnosis of ALS according to El-Escorial criteria and seventeen age-matched controls received a high resolution anatomical T1 scan. Results In ALS patients regional grey matter volume (GMV) reductions were found in the pre- and postcentral gyrus bilaterally which extended to premotor, parietal and frontal regions bilaterally compared with controls (p < 0.05, corrected for the entire volume). The revised ALS functional rating scale showed a positive correlation with GMV reduction of the right medial frontal gyrus corresponding to the dorsolateral prefrontal cortex. No significant differences were found for white matter volumes or when grey and white matter density images were investigated. There were no further correlations with clinical variables found. Conclusion In ALS patients, primary sensorimotor cortex atrophy can be regarded as a prominent feature of the disease. Supporting the concept of ALS being a multisytem disorder, our study provides further evidence for extramotor involvement which is widespread. The lack of correlation with common clinical variables probably reflects the fact that heterogeneous disease processes underlie ALS. The discrepancy within all published morphometric studies in ALS so far may be related to differences in patient cohorts and several methodological factors of the data analysis process. Longitudinal studies are required to further clarify the time course and distribution of grey and white matter pathology during the course of ALS.
Frontotemporal white matter changes in amyotrophic lateral sclerosis
Abstract Cognitive dysfunction can occur in some patients with amyotrophic lateral sclerosis (ALS) who are not suffering from dementia. The most striking and consistent cognitive deficit has been found using tests of verbal fluency. ALS patients with verbal fluency deficits have shown functional imaging abnormalities predominantly in frontotemporal regions using positron emission tomography (PET). This study used automated volumetric voxel-based analysis of grey and white matter densities of structural magnetic resonance imaging (MRI) scans to explore the underlying pattern of structural cerebral change in nondemented ALS patients with verbal fluency deficits. Two groups of ALS patients, defined by the presence or absence of cognitive impairment on the basis of the Written Verbal Fluency Test (ALSi, cognitively impaired, n=11; ALSu, cognitively unimpaired n=12) were compared with healthy age matched controls (n=12). A comparison of the ALSi group with controls revealed significantly (p<0.002) reduced white matter volume in extensive motor and non-motor regions, including regions corresponding to frontotemporal association fibres. These patients demonstrated a corresponding cognitive profile of executive and memory dysfunction. Less extensive white matter reductions were revealed in the comparison of the ALSu and control groups in regions corresponding to frontal association fibres. White matter volumes were also found to correlate with performance on memory tests. There were no significant reductions in grey matter volume in the comparison of either patient group with controls. The structural white matter abnormalities in frontal and temporal regions revealed here may underlie the cognitive and functional imaging abnormalities previously reported in non-demented ALS patients. The results also suggest that extra-motor structural abnormalities may be present in ALS patients with no evidence of cognitive change. The findings support the hypothesis of a continuum of extra-motor cerebral and cognitive change in this disorder.
Global brain atrophy and corticospinal tract alterations in ALS, as investigated by voxel-based morphometry of 3-D MRI
Corpus callosum atrophy in amyotrophic lateral sclerosis
Abstract Recent studies have suggested widespread involvement of the cerebral regions other than the primary motor cortex in amyotrophic lateral sclerosis. To investigate atrophy of the corpus callosum as a measure of cerebral pathology, we studied 25 right-handed patients with sporadic amyotrophic lateral sclerosis using magnetic resonance imaging. Five patients had cognitive decline or emotional and personality changes. The ratios of mid-sagittal corpus callosum areas to the midline internal skull surface area on T1-weighted images were analysed. Compared with 25 age- and sex-matched right-handed control subjects, the patients had significantly decreased callosal/skull area ratio, with anterior predominance of the degree of atrophy. The patients with cognitive decline or psychiatric symptoms had substantial atrophy of the anterior fourth of the corpus callosum. These findings suggest that atrophy of the corpus callosum, especially in the anterior half, is present in amyotrophic lateral sclerosis, and that severe atrophy in the anterior fourth is associated with cognitive decline and psychiatric symptoms. Callosal atrophy may reflect the widespread distribution of pathological changes in the cerebral cortex, which are accentuated in the frontal cortex.
Amygdala size in amyotrophic lateral sclerosis without dementia: an in vivo study using MRI volumetry
pAbstract/p pBackground/p pEvidence for extra-motor involvement in non-demented patients with amyotrophic lateral sclerosis (ALS) has been provided by multiple studies, in particular neuropathological studies have demonstrated neuronal loss in the amygdala. The aim of this study was to investigate possible alterations of amygdala volumes itin vivo/it./p pMethods/p pTwenty-two moderately disabled patients with definite ALS without cognitive or behavioural deficits and 22 age-matched healthy controls were included. Amygdala and total brain volumes were measured by region-of-interest-based volumetry in 3-D MRI./p pResults/p pA trend was observed with reduced amygdala size in the ALS group, since mean absolute and brain size-corrected amygdala volumes were 6.9% and 7.6% lower in the patient group compared to those in normal controls (P = 0.086 and P = 0.110), respectively./p pConclusion/p pVolumetrically identifiable alterations of the amygdala can be mapped itin vivo /itand may be associated with psychopathological findings in later stages of ALS./p
Involvement of the caudate nucleus head and its networks in sporadic amyotrophic lateral sclerosis-frontotemporal dementia continuum
We investigated common structural and network changes across the sporadic amyotrophic lateral sclerosis (ALS)-frontotemporal dementia (FTD) continuum. Based on cluster analysis using the frontotemporal assessment battery, 51 patients with sporadic ALS were subdivided into three groups: 25 patients with ALS with cognitive deficiency (ALS-CD); seven patients who satisfied FTD criteria (ALS-FTD), and 19 patients with ALS with normal cognitive function (ALS-NC). Compared with the controls, gray matter images from patients with ALS-FTD showed atrophic changes in the following order of severity: caudate head, medial frontal gyrus, thalamus, amygdala, putamen, and cingulate gyrus (peak level, uncorrected p < 0.001). The caudate head was significant at the cluster level using FWE correction (p < 0.05). Diffusion tensor imaging with tract-based spatial statistics revealed white matter changes in the areas surrounding the caudate head, the internal capsule, and the anterior horn of the lateral ventricle in the ALS-CD and ALS-FTD. Probabilistic diffusion tractography showed a significant decrease in structural connectivity between the caudate head and the dorsomedial frontal cortex and the lateral orbitofrontal cortex, even in the ALS-NC. Our results indicated that the caudate head and its networks were the most vulnerable to lesion in sporadic ALS-FTD-spectrum patients associated with cognitive decline with FTD features.
Whole-brain and regional brain atrophy in amyotrophic lateral sclerosis
Recent evidence from neuropsychologic and neuroimaging studies suggests that central nervous system involvement in amyotrophic lateral sclerosis (ALS) extends beyond motor neurons. Our purpose was to obtain measures of global and regional atrophy in nondemented patients with ALS to assess subtle structural brain changes.MR images, acquired from 16 patients and 9 healthy subjects (HS), were processed by using the Structural Imaging Evaluation of Normalized Atrophy (SIENA) software to estimate whole-brain atrophy measures and the voxel-based morphometry (VBM) method to highlight the selective volumetric decrease of single cerebral areas. In addition, each subject underwent a neuropsychologic examination.In patients with ALS, brain parenchymal fraction was slightly lower compared with HS (P = .012), and seemed to be related to the presence of cognitive impairment. Patients showed a gray matter volume decrease in several frontal and temporal areas bilaterally (P < .001 uncorrected) compared with HS, with a slight prevalence in the right hemisphere. No volume reduction in primary motor cortices of patients was detected. Performances on Symbol Digit Modalities Test were significantly worse in patients compared with HS (P = .025).The presence of mild whole-brain volume loss and regional frontotemporal atrophy in patients with ALS could explain the presence of cognitive impairment and confirms the idea of ALS as a degenerative brain disease not confined to motor system.
Voxel-wise meta-analysis of gray matter changes in amyotrophic lateral sclerosis
Background:Increasing neuroimaging studies have revealed gray matter (GM) anomalies of several brain regions by voxel-based morphometry (VBM) studies in patients with amyotrophic lateral sclerosis (ALS). A voxel-wise meta-analysis was conducted to integrate the reported studies to determine the consistent GM alterations in ALS based on VBM methods. Methods:Ovid Medline, Pubmed, Emabase, and BrainMap database were searched for relevant studies.Data were extracted by two independent researchers. Voxel-wise meta-analysis was performed using the effect-size signed differential mapping (ES-SDM) software. Results:Twenty-nine VBM studies comprising 638 subjects with ALS and 622 healthy controls (HCs) met inclusion criteria.The global GM volumes of ALS patients were significantly decreased compared with those of HCs. GM reductions in patients were mainly located in the right precentral gyrus, the left Rolandic operculum, the left lenticular nucleus and the right anterior cingulate/paracingulate gyri. The right precentral gyrus and the left inferior frontal gyrus might be potential anatomical biomarkers to evaluate the severity of the disease, and longer disease duration was associated with more GM atrophy in the left frontal aslant tract and the right precentral gyrus in ALS patients. Conclusion:The results support that ALS is a complex degenerative disease involving multisystems besides the motor system.The mechanism of asymmetric atrophy of the motor cortex and the implication of Rolandic operculum involvement in ALS need to be further elucidated in future studies.
Motor and extra-motor gray matter atrophy in amyotrophic lateral sclerosis: quantitative meta-analyses of voxel-based morphometry studies
Considerable evidence from previous voxel-based morphometry studies indicates widespread but heterogeneous gray matter (GM) deficits in amyotrophic lateral sclerosis (ALS). Here, we aimed to investigate the concurrence across voxel-based morphometry studies to help clarify the spatial pattern of GM abnormalities that underlie this condition. Comprehensive meta-analyses to assess regional GM anomalies in ALS were conducted with the Anisotropic Effect Size version of Signed Differential Mapping software package. Twenty studies, which reported 22 comparisons and were composed of 454 ALS patients and 426 healthy controls, were included in the meta-analyses. Regional GM atrophy in ALS was consistently found in the frontal, temporal, and somatosensory areas. Meta-regression demonstrated that the disease duration, disease severity, and age were significantly related to GM deficits in ALS patients. The present meta-analysis provides convergent evidence that ALS is a multisystem degenerative disorder that is accompanied by a unique and widespread pattern of robust cortical GM atrophy. Future studies should investigate whether this atrophy pattern is a diagnostic and prognostic marker.
Grey matter volume changes over the whole brain in amyotrophic lateral sclerosis: a voxel-wise meta-analysis of voxel based morphometry studies
Amyotrophic lateral sclerosis (ALS) is a progressive neurodegenerative disease with selected both upper and lower motor neuron involvement. Although some inconsistent results exist, both pathological studies and many structural neuroimaging studies have revealed brain volume changes in ALS. To provide an objective overview of structural changes in ALS, a voxel-wise meta-analysis was performed in published voxel based morphometry (VBM) studies. A systematic search of VBM studies was applied in ALS. Five studies met the inclusion criteria, comprising 84 ALS patients and 81 normal controls. A voxel-wise meta-analysis was performed on the retrieved VBM studies using signed differential mapping. Descriptive analysis showed that 25% of ALS patients had right precentral gyrus atrophy (2373 voxels). Group analysis demonstrated regional grey matter loss over the whole brain in the right precentral gyrus (p = 7.96 0103 100908084). Sensitivity analysis showed good sensitivity (157 voxels). In conclusion, right precentral grey matter atrophy was a common finding and prominent feature of brain structural changes in ALS.
El Escorial ####: FFFF criteria for the diagnosis of amyotrophic lateral sclerosis
(2000). El Escorial revisited: Revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotrophic Lateral Sclerosis and Other Motor Neuron Disorders: Vol. 1, No. 5, pp. 293-299.
New ideas on the ALS functional rating scale
Handbook of Neurologic Rating Scales
Handbook of neurologic rating scales edited by Robert M. Herndon Demos Vermande, 1997
Mini-Mental State Examination (MMSE)
Voxel-based morphometry—the methods
Unchanged total number of neurons in motor cortex and neocortex in amyotrophic lateral sclerosis: a stereological study
Modern stereological methods provide precise and reliable estimates of the number of neurons in specific regions of the brain. The total number of neurons in the neocortex and motor cortex from eight patients suffering from amyotrophic lateral sclerosis (ALS) and nine controls was estimated. No attempt was made to estimate subpopulations of neurons such as the number of giant pyramidal cells of Betz. No difference was found in the average number of neurons in neocortex in ALS and controls, 21.7 and 22.3脳10 9 , respectively, and 1.33 and 1.29脳10 9 in motor cortex, respectively. In the light of our stereological measurements, results obtained from in-vivo proton magnetic resonance spectroscopy ( 1 H-MRS), suggesting neuronal loss in ALS, may instead be due to neuronal metabolic dysfunction and/or alteration in the size or the volume fraction of the neurons.
Changes in shapes of surviving motor neurons in amyotrophic lateral sclerosis
In , motor neurons in the spinal cord and brainstem shrink before they die. In 12 cases of sporadic , and in 11 control subjects, we have measured the neurons in the second sacral segment and the hypoglossal , and have calculated a 'shape index' that shows the convexity or concavity of the . (The shape index, SI = 100 x C/P, where C is the circumference of the largest circle that can be inscribed in the neuron and P is the perimeter of the perikaryon, including the bases of the dendrites as seen in a Nissl preparation. The shape index increases with increasing convexity of the cell.) In the ventral horn of segment S2 and in the hypoglossal , the surviving motor neurons in showed significantly decreased size and increased shape index (convexity) of the . By contrast, the of Onuf in segment S2, consisting of neurons that supply the pelvic floor muscles, was preserved in . Its cells did not differ significantly in size or convexity between the and control groups. In both the hypoglossal and S2 neuronal populations in , the sizes of the cells were positively correlated with the numbers of surviving motor neurons. However, there was no correlation of the shape index with numbers of cells. This is interpreted as due to shrinkage of neurons still taking place at the time of , when the changes in shape were probably largely completed. These observations indicate that the mechanism of neuronal atrophy in may involve both reduced protein synthesis and enzymatic degradation of the within the larger dendrites.
Cognitive function in bulbar- and spinal-onset amyotrophic lateral sclerosis. a longitudinal study in 52 patients
Decreased thickness of primary motor cortex in primary lateral sclerosis
BACKGROUND AND PURPOSE: () is a rare form of characterized by upper motor neuron dysfunction. Because pathologic examination has revealed a loss of neurons in the motor cortex of patients with , we sought to confirm and extend this finding by using imaging to measure cortical thickness.: Seven patients with and 7 age-matched neurologically normal control subjects were examined with heavily T1-weighted short-inversion recovery (STIR) imaging performed at 3T. Cortical thickness in the anterior and posterior banks of both the central and precentral sulci were measured.: Primary motor cortex (M1) was significantly thinner in patients with than M1 in healthy control subjects, measuring 2.32 +/- 0.21 mm compared with 2.79 +/- 0.18 mm (P =.0008). Cortical thickness did not differ between the 2 groups for primary sensory cortex or for the anterior or posterior banks of the precentral sulcus. Therefore, loss of gray matter was specific to motor cortex. Although this difference was modest, cortical thickness discriminated between the 2 groups; only 1 PLS case was within the range of normal measurements.: Decreased thickness of M1 on the anterior bank of the precentral sulcus in patients with , demonstrable by imaging, indicates a selective loss of upper motor neurons in this disease. Measurements of cortical thickness by imaging may provide a useful biomarker for diagnosis and study of .
Detection of motor cortex thinning and corticospinal tract involvement by quantitative MRI in amyotrophic lateral sclerosis
URL
PMID:1862277218622772
[本文引用: 1]

We prospectively investigated pathological modifications in the corticospinal tract (CST), by diffusion tensor imaging (DTI) in 14 patients with sporadic amyotrophic lateral sclerosis (ALS) and 12 healthy volunteers. We used a validated automated method to accurately measure the in vivo thickness of the cerebral cortex. We found a reduction of precentral cortical ribbon thickness in ALS patients with respect to control subjects. DTI metrics demonstrated disorganization of the CST, as characterized by decreased fractional anisotropy (FA) and increased Apparent Diffusion Coefficient in ALS patients with respect to control subjects. Decreased mean FA values along the CST significantly correlated with clinical measures of pyramidal and bulbar impairment.
A voxel-based morphometry study of patterns of brain atrophy in ALS and ALS/FTLD
Involvement of the frontotemporal lobe and limbic system in amyotrophic lateral sclerosis: as assessed by serial computed tomography and magnetic resonance imaging
The present paper concerns serial examinations of computed tomography (CT) and magnetic resonance imaging (MRI) in 22 patients with sporadic amyotrophic lateral sclerosis (ALS). Supranuclear ophthalmoplegia developed in 13 and dementia in 3 patients. The investigations showed gradually progressive atrophy, first in the frontal and anterior temporal lobes then in the precentral gyrus, and later in the postcentral gyrus, anterior part of the cingulate gyrus, corpus callosum and brain stem tegmentum. MRI revealed high intensity signals on T2-weighted images in the precentral and adjacent gyri, frontotemporal white matter and pyramidal tract as well as rarely in the globus pallidus and thalamus. These neuroradiological changes were not related to the duration of the clinical course or to the degree of the motor impairment. These alterations may play a critical role in the supranuclear ophthalmoplegia seen in ALS patients. The dementia of ALS probably reflects involvement of both the frontotemporal lobes and limbic system.
Alzheimer disease pathology in amyotrophic lateral sclerosis
Amyotrophic lateral sclerosis (ALS) is characterized by degeneration of upper and lower motor neurons. In some ALS patients, dementia or aphasia may be present (ALS-D). The dementia is most commonly a frontotemporal dementia (FTD), and many of these cases have ubiquitin-positive, tau-negative inclusions in neurons of the dentate gyrus and superficial layers of the frontal and temporal lobes. Identical inclusions have been found in cases presenting with FTD and have been designated motor neuron disease (MND)-inclusions. Cases of ALS-D without MND-inclusions have been reported to show neocortical gliosis, neuronal loss, and superficial spongiosis, but there have also been scattered case reports of ALS with Alzheimer鈥檚 disease (AD). To determine whether AD pathology may play a role in the dementia or aphasia syndromes in ALS, we reviewed 30 cases of sporadic ALS diagnosed at the University of Pittsburgh Medical Center. A clinical history of ALS-D was found in 24.1% of the cases, of which 57% had MND-inclusions. Although the ALS-D cases with MND-inclusions typically had amyloid-beta (A尾) plaques, there were no neuritic plaques. Three cases of ALS-D had no MND-inclusions, and two of these fulfilled pathological criteria for AD. One ALS-D case showed severe amyloid angiopathy but no neuritic plaques or MND-inclusions. MND-inclusions were not found in any ALS case without dementia; however, four patients without dementia or aphasia showed moderate or frequent numbers of neuritic plaques. In conclusion, we found that approximately 30% of ALS cases with dementia have AD and that some ALS cases without frank dementia have significant AD pathology.
Pathology of amyotrophic lateral sclerosis
ABSTRACT Motor neuron disease (MND) is used in this paper as the generic label, encompassing the clinical variants of amyotrophic lateral sclerosis (ALS), progressive myelopathic muscular atrophy (PMMA), and progressive bulbar palsy (PBP). ALS is limited to instances of anterior horn cell plus pyramidal tract involvement. When only anterior horn cell lesions are inferred, either PMMA or PBP is used, depending on the levels of involvement; when both cord and brain stem are affected. PBP is the designation. Mortality data on MND have been available for a number of countries since 1949. The coding used under international rules has varied considerably over this interval. Before 1969, hereditary muscular atrophies were included. Since 1979, no subdivision by type of MND is possible. International death rates for MND have all been rather close to 1 per 100,000 population per year, though perhaps nearer to 1.4 on the average in recent years. There has been an increasing proportion of MND deaths coded to ALS between 1949 and 1977. There is no notable geographic variation among countries, nor within countries such as the U.S. and Denmark. A slight upward trend in death rates over time in the U.S. is matched by a slight decrease in Denmark. Death rates from all sources indicate a male preponderance for ALS or MND as a whole, at about 1.5 to 1, male to female. There is also a consistent predilection by age, with few deaths under age 50 or so and a clear maximum in age-specific death rates at about age 70. This holds for both sexes. In the U.S., there is also a white-nonwhite difference, with a ratio of about 1.6:1 but with age and sex differences similar to whites. Average annual incidence rates from among white occidental populations range mostly between 0.6 and 1.8 per 100,000 population for MND and about 0.8 and 1.5 per 100,000 for ALS. Again a male predilection is seen. There is a clear maximum in age-specific incidence rates at about age 65 in all surveys except that of Rochester, Minnesota, where the age-specific rate for those 75+ years of age is apparently higher than that for those age 65 to 74. Incidence rates, then, are quite similar one land to another. A reported deficit in Mexico may reflect case-selection bias. An excess among Filipinos on Hawaii seems more a function of population age-distributions than a true racial or ethnic difference. Prevalence rates from outside the Orient range from about 1 to 7 per 100,000 population for MND and about 2 to 7 for ALS. Those surveys more likely to be reasonably complete provide ALS prevalence rates of about 4 to 6, and an overall estimate of ALS prevalence of some 5 per 100,000 population is a reasonable figure. In the Orient, most of the MND prevalence rates fall within the same range as in the occident, except for two areas of the Kii peninsula of southern Honshu, Japan, where the reported prevalence rates are some 100 to 200 per 100,000 population. These cases are similar to the Guamanian ALS, both clinically and pathologically...
Motor neuron diseases: comparison of single-voxel proton MR spectroscopy of the motor cortex with MR imaging of the brain
To evaluate single-voxel proton magnetic resonance (MR) spectroscopy in detection of abnormality of the upper motor neuron in patients with motor neuron diseases.In 43 of 50 patients with motor neuron disease and 14 of 14 control subjects, matching sets of MR spectra were obtained in the left and right motor cortex. The ratio of N-acetylaspartate (NAA) to creatine (Cr) was derived from peak area measurements. Mean ratios were calculated for control subjects and several patient groups, including patients with amyotrophic lateral sclerosis (ALS) or primary lateral sclerosis (PLS). MR images were evaluated for corticospinal tract hyperintensity and central sulcus dilatation.Mean NAA/Cr values were significantly different between control subjects and the ALS or PLS groups (P < .05). With an optimal cutoff of 2.5, NAA/Cr values were abnormal in 15 (79%) of 19 patients with ALS, 12 (67%) of 18 patients with PLS, and one (7%) of 14 control subjects. Corticospinal tract hyperintensity, central sulcus enlargement, or both were found in 43% of the ALS group, 24% of the PLS group, and 7% of the control group.NAA/Cr values determined at single-voxel proton MR spectroscopy are more sensitive than are standard findings at MR imaging in the detection of upper motor neuron disease.
Jr., et al. Volumetric analysis reveals corticospinal tract degeneration and extramotor involvement in ALS
Abstract BACKGROUND: Pathologic changes in the motor cortex and corticospinal tracts in ALS may be reflected by abnormal signal intensities on conventional MRI. The sensitivity of these changes in detecting underlying pathology remains unclear. METHOD: The authors used automated image analysis to quantify volumes of cerebral gray and white matter in 16 patients with ALS (eight limb onset, eight bulbar onset) and eight normal controls. Previously they had demonstrated a reduction in N-acetyl aspartate/creatine + phosphocreatine (NAA/[Cr + PCr]) measured by (1)H-MRS in the subcortical white matter in the motor cortex region in the patients with bulbar-onset ALS. To determine whether this resulted from axonal degeneration, they also compared gray and white matter volumes in the patients with limb- and bulbar-onset ALS. RESULTS: There were no differences in the total brain volumes of gray or white matter for the three subject groups (p > 0.23). Comparison of the total ALS group and controls revealed localized deficits in gray matter volume centered on Brodmann areas 8, 9, and 10 bilaterally. Comparison of the patients with limb- and bulbar-onset ALS revealed deficits in the white matter volume in the bulbar-onset group, extending bilaterally from the precentral gyrus into the internal capsule and brainstem, consistent with the course of the corticospinal tract. There was no loss in gray matter volume in the precentral gyri. CONCLUSIONS: The loss of gray matter in the frontal regions (total ALS group) provides further support that ALS is a multisystem disorder. In addition, there is in vivo evidence of axonal degeneration in the subcortical white matter in the motor region in patients with bulbar-onset ALS. This is consistent with a "dying back" process affecting cortical motoneurons in bulbar-onset ALS.
The size distribution of neurons in the motor cortex in amyotrophic lateral sclerosis
Abstract The motor cortex of eight patients with amyotrophic lateral sclerosis (ALS) and nine control subjects was used in the study. Recent stereological tools, the disector and the rotator method, were applied to the motor cortex of patients with ALS and control subjects to obtain estimates of mean perikaryon volume, mean neuronal nuclear volume, total perikaryon volume and total neuronal nuclear volume. No significant differences were found in any of the estimates. In vivo proton magnetic resonance spectroscopy studies show a decrease in the concentration of neuronal markers. We expected to find changes in perikaryon and/or nuclei neuronal volume because the total neuron number is unchanged in ALS compared with control subjects. However, this was not the case; our results suggest that metabolic changes take place in the motor cortex of ALS patients without these concomitant anatomical changes.
Left inferior frontal gyrus is critical for response inhibition
Background Lesion studies in human and non-human primates have linked several different regions of prefrontal cortex (PFC) with the ability to inhibit inappropriate motor responses. However, recent functional neuroimaging studies have specifically implicated right inferior PFC in response inhibition. Right frontal dominance for inhibitory motor control has become a commonly accepted view, although support for this position has not been consistent. Particularly conspicuous is the lack of data on the importance of the homologous region in the left hemisphere. To investigate whether the left inferior frontal gyrus (IFG) is critical for response inhibition, we used neuropsychological methodology with carefully characterized brain lesions in neurological patients. Results Twelve individuals with damage in the left IFG and the insula were tested in a Go/NoGo response inhibition task. In alternating blocks, the difficulty of response inhibition was easy (50% NoGo trials) or hard (10% NoGo trials). Controls showed the predicted pattern of faster reaction times and more false alarm errors in the hard condition. Left IFG patients had higher error rates than controls in both conditions, but were more impaired in the hard condition, when a greater degree of inhibitory control was required. In contrast, a patient control group with orbitofrontal cortex lesions showed intact performance. Conclusion Recent neuroimaging studies have focused on a highly specific association between right IFG and inhibitory control. The present results indicate that the integrity of left IFG is also critical for successful implementation of inhibitory control over motor responses. Our findings demonstrate the importance of obtaining converging evidence from multiple methodologies in cognitive neuroscience.
Role of the contralateral inferior frontal gyrus in recovery of language function in poststroke aphasia: a combined repetitive transcranial magnetic stimulation and positron emission tomography study
Involvement of left inferior frontal gyrus in sentence-level semantic integration
Using event-related functional MRI, we examined the involvement of the left inferior frontal gyrus (LIFG) in semantic integration in reading Chinese sentences. During scanning, Chinese readers read individually presented sentences and judged whether or not a sentence was semantically acceptable. Behaviorally, those sentences with a small degree of semantic violation were found to be more difficult to reject relative to sentences with a large degree of semantic violation, indicating that more semantic integration occurred in the former than in the latter condition. Direct contrast revealed significantly greater brain activity in the LIFG for sentences with a small violation, relative to those with a large violation, but no differences in any anterior temporal cortical areas between the two types of anomalous sentences. The results are in line with the idea that the LIFG plays a critical role in integrating individual word meanings to coherent sentence-level messages, but not with the idea that semantic integration depends on anterior temporal cortex in language comprehension.
Functional heterogeneity of left inferior frontal cortex as revealed by fMRI
Are amyotrophic lateral sclerosis patients cognitively normal?
Patients with ALS are often told that the disease spares cognition; however, recent evidence suggests deficits in frontal executive skills occur in a sizable minority of ALS patients. In many instances, the frontal executive deficits represent the co-occurrence of frontotemporal lobar dementia (FTLD) and ALS. Word generation, a simple frontal task that takes <2 minutes, was tested in 100 consecutive patients with ALS seen in the authors' multidisciplinary clinic. Any patient with a prior dementia diagnosis was excluded from the study. A subset of 44 patients agreed to undergo further neuropsychological testing and clinical interview to confirm or deny a diagnosis of dementia. Diminished word generation was found in one-third. Of the patients with abnormal word generation who agreed to further evaluation, nearly all were shown to meet research criteria for FTLD. In addition, one-quarter of the patients with normal word generation who agreed to further evaluation met research criteria for FTLD; these patients had new-onset personality changes. This study suggests that frontal executive deficits are present in half of ALS patients, many of whom meet strict research criteria for FTLD. Word generation tests are a useful screening tool in this cohort.
Memory deficits and retrieval processes in ALS
Abstract Subtle neuropsychological deficits have been described in patients affected by amyotrophic lateral sclerosis (ALS) without dementia. Overall, selective impairment in memory function has been reported, but the source of memory impairment in ALS has yet to be defined. We performed neuropsychological screening in 20 ALS patients. Semantic encoding and post-encoding cue effects on the retrieval of word lists were investigated in the ALS patients and normal controls. Severity of memory impairment was correlated to cerebral blood perfusion detected by single photon emission computed tomography (SPECT). ALS patients showed moderate impairments in frontal and memory tests. Short-term memory was normal, while serial position retrieval of word lists with normal recency effect but poor primacy effect showed long-term memory deficit. ALS patients performed better in cued encoding than in cued post-encoding recall condition. In the cued post-encoding condition, the primacy effect in word list recall improved significantly in controls, but not in ALS patients, as compared with both the free recall and cued encoding conditions. SPECT hypoperfusion was observed in frontal and temporal areas in ALS patients. ALS patients showed a long-term memory deficit which did not improve in cued post-encoding condition as it does for controls. We hypothesize abnormal retrieval processes related to frontal lobe dysfunction which entails difficulties in generating stable long-memory traces at encoding.
Word retrieval in amyotrophic lateral sclerosis: a functional magnetic resonance imaging study
The cognitive impairment revealed in some non- demented amyotrophic lateral sclerosis (ALS) patients is characterized by executive dysfunction with widely repeated deficits on tests of verbal (letter) fluency. However, conflicting evidence exists of an impairment on other word retrieval tasks, such as confrontation naming, which do not place heavy demands on executive processes. Previous research has demonstrated intact confrontation naming in the presence of verbal fluency deficits, although naming deficits have been described in other studies. In this investigation, functional MRI (fMRI) techniques were employed to explore whether word retrieval deficits and underlying cerebral abnormalities were specific to letter fluency, which are more likely to indicate executive dysfunction, or were also present in confrontation naming, indicating language dysfunction. Twenty-eight non-demented ALS patients were compared with 18 healthy controls. The two groups were matched for age, intelligence quotient, years of education, and anxiety and depression scores. Two compressed-sequence overt fMRI activation paradigms were employed, letter fluency and confrontation naming, which were developed for use with an older and potentially impaired population. In ALS patients relative to controls, the letter fluency fMRI task revealed significantly impaired activation in the middle and inferior frontal gyri and anterior cingulate gyrus, in addition to regions of the parietal and temporal lobes. The confrontation naming fMRI task also revealed impaired activation in less extensive prefrontal regions, including the inferior frontal gyrus and regions of the temporal, parietal and occipital lobes. These changes were present despite matched performance between patients and controls during each activation paradigm. The pattern of dysfunction corresponded to the presence of cognitive deficits on both letter fluency and confrontation naming in the ALS group. This study provides evidence of cerebral abnormalities in ALS in the network of regions involved in language and executive functions. Moreover, the findings further illustrate the heterogeneity of cognitive and cerebral change in ALS.
Amyotrophic lateral sclerosis
Cognitive impairment in motor neuron disease with bulbar onset
Abstract METHODS: Twenty-three patients with bulbar onset motor neuron disease/amyotrophic lateral sclerosis (MND/ALS) were clinically assessed. They subsequently underwent serial neuropsychological testing, event-related potentials (ERP) and SPECT studies. Cognitive impairment was defined by clinical evidence of dementia (DSM-IV and frontal evaluation) or by significant alteration indicated by neuropsychological testing (excluding patients with depression and major anxiety), or both. RESULTS: Eleven patients (48%) were found to be cognitively impaired. Abnormalities indicated fronto-temporal involvement, with memory impairment, alteration of judgement and reasoning, reduced speech, behavioural dyscontrol and alteration of daily living activities. This impairment correlated well with event-related potentials and SPECT studies. Event-related potentials were the most sensitive test as 100% of the impaired patients had abnormal ERP (p = 0.04). The cognitively impaired group differed from the other group mainly by gender ratio (male/female) with an important male predominance: 1.75 vs. 0.33. MND/ALS was also more severe when cognitive decline was present. CONCLUSION: This study adds further arguments for a cognitive impairment in MND/ALS. This also reinforces the hypothesis that there is continuum between MND/ALS and fronto-temporal lobe dementia.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}