

CORONARY artery bypass grafting (CABG) is one of the most effective treatments to ensure myocardial re-perfusion for the advanced coronary artery atherosclerotic heart disease. More than 9 800 patients with coronary heart disease accept CABG operation annually in China.1 Some patients present with symptoms after operation, such as recurrent angina or effort dyspnea. It was reported that graft stenosis and closure occurred in 20%-30% of patients within 3 years after CABG operation.2 Therefore, it is imperative to accurately assess the graft patency after CABG operation.
Invasive cardiac angiography (ICA) has been the gold standard to evaluate graft patency; however, despite its invasive nature, the procedures also accompany with complications, such as thrombosis, dissection, arrhythmia, myocardial infarction and stroke.3 In recent years, 64 slice multi-detector computed tomography (MDCT) has emerged as an alternative to ICA in evaluating the graft and native coronary arteries for its diagnostic potentials, low cost and safety.4 Some studies5-8 have shown that 64-MDCT has high sensitivity, specificity, positive predictive value and negative predictive values in evaluation of graft patency in patients with CABG operation compared with ICA.
In the meantime, there hasn't sufficient data to identify the risk factors that affect the graft patency. A few studies reported conflicting findings.9-12 Levisman JM et al 9 found that the comorbidity of diabetes had no significant impact on the graft failure. However, Yanagawa B and Singh SK et al 10, 11 found that diabetes was a potential clinical predictor for the development of graft failure. Choi JS et al 12 reported that diabetes mellitus did not affect the early and midterm postoperative outcome. Although the type of graft (i.e. vein or artery) was also reported to affect the long-term outcome of CABG,13 little has been known regarding the impact of distant anastomosis site on graft patency. As a result, in the present study, we aimed to evaluate the CABG graft patency in different graft types and different distant anastomosis site by using 64-slice MDCT, and secondly, to identify the risk factors that affect the midterm graft failure among the clinical and imaging characteristics of the patients.
MATERIAL AND METHODS
Patients and information collection
The retrospective study was approved by the institutional ethic review board, and the consents from patients were waived. From August 2012 to December 2015, consecutive patients with history of CABG who underwent postoperative follow-up examination using 64-MDCT to determine the outcomes of grafts in our institute were reviewed. Subjects who didn’t undergo postoperative MDCT angiography due to renal disfunction, arrhythmia, allergic to iodinated contrast media, or failed to accomplish a 15-second breath hold were excluded. Subjects who had poor MDCT image quality due to remarkable artifacts were also excluded. We collected the basic information of the enrolled patients, including age, gender, height, weight, symptoms at the MDCT examination, comorbidities of type 2 diabetes, hypertension, dyslipidemia, history of smoking, and cerebrovascular disease, ongoing medication, date of coronary artery bypass graft surgery, date of 64-MDCT examination, preoperative quantitative coronary angiography results. The operative notes were carefully reviewed to extract the information on the graft type, number of all graft conduits, and the target anastomosis for analysis.
Coronary artery imaging
Coronary CT angiography(CTA) was performed on a 64-slice CT scanner (SOMATOM Sensation Cardiac 64, Siemens Medical System, Forchheim, Germany). Each patient received 85ml contrast media (Omnipaque 350 mg I/ml, GE Healthcare, Pewaukee, WI) intravenously at a rate of 5ml/s, followed by 40ml saline solution at the same rate. Bolus tracking technique was used to monitor the intensity of aortic root and trigger the scan protocol automatically when the CT attenuation of aortic root reached 150 HU. Scanning field was set from thoracic inlet to costophrenic angles. For patients with heart rates less than 65bpm, CTA was performed using a prospective ECG-triggering protocol with tube voltage 120kV, effective tube current 195mAs. Otherwise, a retrospective ECG-triggering protocol was used with parameters of 0.33 s/r, 120kV, eff.900mAs, pitch 0.18, slice collimation 64x0.6 mm, thickness 0.75 mm. Axial images were reconstructed using standard reconstruction algorithm with a slice thickness of 1 mm (increment of 0.6 mm) at the optimal ECG-phases when the minimum motion artifacts presented on the images for optimal delineation of each coronary artery bypass graft and main branch of the coronary arteries.
Post-processing and analysis of images
For each patient, the axial image data were transferred to an Advanced Workstation (Circulation 2 workstation, Siemens, Forchheim, Germany) for post-processing and vessels reconstruction. The CABG was reformatted with Volume Render (VR), maximum intensity projection (MIP), multi-planar reconstruction (MPR) or curved planar reconstruction (CPR). MPR and CPR images were predominantly used to assess the CABG patency.
Two experienced radiologists reviewed the MDCT images independently to identify the graft patency with reference of brief operation records on graft number and anastomosed location. The graft patency status was classified into 2 categories according to the imaging findings: patent (excellent visualization, luminal stenosis<50%), and poor patent (visualized with significant stenosis, luminal stenosis ≥50%, or totally occluded).13 Luminal stenosis was quantified by the formula: (diameterproximal normal lumen-diameterstenosed lumen) /diameterproximal normal lumen. In case of sequential bypass graft with multiple target anastomoses, each sequential bypass graft was considered as isolate grafts. The graft targets were divided into three territories: left anterior descending branch (LAD), including the diagonal branch (D); left circumflex coronary artery (LCX), including obtuse marginal branch (OM); right coronary artery (RCA), including posterior descending artery (PDA) and posterior lateral branch (PLB). For any discrepancy in interpreting, a consensus was achieved by discussion between the two radiologists.
Statistical analysis
The clinical characteristics of patients, including age, gender, history of diabetes, hypertension, dyslipidemia, smoking, cerebrovascular disease, ongoing medical therapy as well as graft type and target territories, were compared between patients with patent grafts and those with poor patent grafts. Continuous variables were described as mean±standard deviation and compared using t test; categorical variables were described as percentages and analyzed using chi-square test. Univariate analysis and multivariate logistic regression analysis were performed to identify the risk factors that were associated with graft failure. A two-tailed P value of <0.05 was considered statistically significant. All the statistical analyses were conducted by SPSS (version 19.0, SPSS Inc, Chicago, IL).
RESULTS
Clinical characteristics
A total of 379 consecutive patients with history of CABG and having completed 64-MDCT follow-up examinations were initially included in this study. All the patients were not referred to redo the CABG. There were 38 patients with 59 bypass grafts excluded for remarkable artifacts on CT images (metal clip in 22 segments, calcification inducing blooming in 5, motion artifact in 21) or deficient contrast enhancement (11 CABG segments). So a total of 894 grafts in 341 patients (mean 2.62 grafts per patient) were included in the study, with 273 males and 68 females, mean age of 62.6±10.2, ranged from 32 to 85 years old. The mean interval time between CABG operations and MDCT examinations was 30.2±17.0 months.
The clinical characteristics of patients who had patent grafts and poorly patent grafts were shown in Table 1. All patients received postoperative antiplatelet medication after CABG surgery, including aspirin (100 mg, daily) and clopidogrel (75 mg,daily) regularly. The adjuvant medication other than antiplatelet were beta blocker, angiotensin-converting-enzyme (ACE) inhibitor, statin and calcium channel blocker. Fifty-four out of 341 (15.8%) patients were symptomatic at the time of MDCT. The symptoms included discomfort of the precordial area, chocking sensation in chest, or short of breath.
Table 1 Clinical characteristics of patients who had patent grafts or poorly patent grafts at the time of MDCT examination (n=341)§
| Clinical characteristics | Patient groups | In total | t or χ2value | Pvalue | |
|---|---|---|---|---|---|
| Patent grafts (n=231) | Poor patent grafts (n=110) | ||||
| Sex | |||||
| Male, n (%) | 188(81.4) | 85(77.3) | 273 | 0.79 | 0.37 |
| Female, n (%) | 43(18.6) | 25(22.7) | 68 | ||
| Age, years | 62.7±10.3 | 62.5±10.0 | 62.6±10.2 | 0.42 | 0.87 |
| Bypass grafts, n (%) | 574 | 320 | 894 | ||
| Body Mass Index | 30.1±5.8 | 30.5±6.1 | 30.2±5.9 | 0.55 | 0.45 |
| History of | |||||
| Diabetes, n (%) | 72(31.2) | 41(37.3) | 113 | 1.25 | 0.26 |
| Hypertension, n (%) | 157(68.0) | 61(55.5) | 218 | 5.06 | 0.025 |
| Dyslipidemia, n (%) | 58(25.1) | 38(34.5) | 96 | 3.28 | 0.07 |
| Smoking, n (%) | 118(51.1) | 48(43.6) | 166 | 1.65 | 0.20 |
| Cerebrovascular disease, n (%) | 28 (12.1) | 26 (23.6) | 54 | 7.41 | 0.006 |
| Post-operative adjuvant medication | |||||
| Beta blocker, n (%) | 101(43.7) | 48(43.6) | 149 | 0.00 | 0.98 |
| ACE inhibitor, n (%) | 58(25.1) | 27(24.5) | 85 | 0.01 | 0.9 |
| Statin, n (%) | 107(46.3) | 49(44.5) | 156 | 0.10 | 0.76 |
| Calcium channel blocker, n (%) | 21(9.1) | 9(8.2) | 30 | 0.08 | 0.78 |
| Symptomatic, n (%) | 39(16.9) | 15(13.6) | 54 | 0.59 | 0.44 |
§:Plus and minus values are means ± SD; MDCT: multi-detector computed tomography; ACE: angiotensin-converting-enzyme.
Patency of left internal mammary artery (LIMA) graft and saphenous veins (SV) graft
Of 894 grafts in 341 patients, there were 330 LIMA grafts and 564 SV grafts. Among the 330 LIMA grafts, 326 grafts were anastomosed to the left anterior descending artery (LAD), 4 to the right coronary artery (RCA). Assessed by the MDCT examination, there were 294/330 LIMA grafts (89.1%) being patent (Fig. 1), of which 292 were anastomosed to LAD and 2 to RCA; there were 36/330 LIMA grafts being poor patent,of which 34 were anastomosed to LAD and 2 to RCA. In 326 LIMA grafts that were anastomosed to LAD, preoperative quantitative coronary angiography showed that the significant luminal stenosis exceeding 90% of proximal target vessel occurred in 268 of 292 patent grafts, while in only 1 of 34 poor patent grafts, the proximal target vessel showing significant luminal stenosis exceeding 90% (χ2=167, P<0.001).
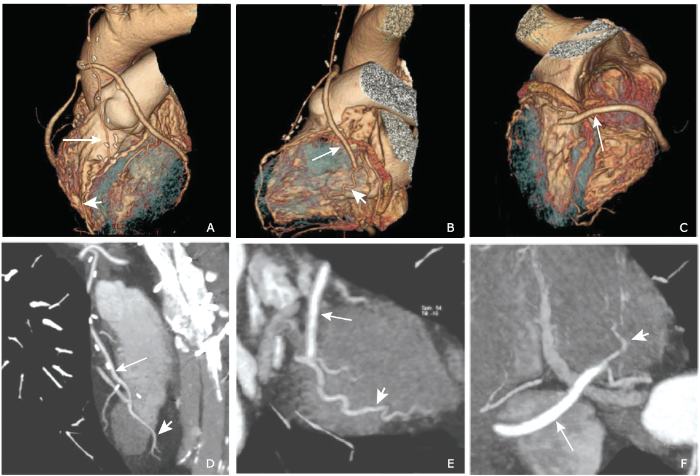
Figure 1.
Volume rendering (VR) and Multi-planar reconstruction (MPR) images of a 72-year-old male who had coronary artery bypass graft (CABG) operation one year ago show the grafts were all patent. A and D, the left internal mammary artery graft (long arrow) was anastomosed to the left anterior descending artery(short arrow); B and E, the saphenous veins graft (long arrow) was anastomosed to the obtuse marginal branch (short arrow); C and F, another saphenous vein graft (long arrow) was anastomosed to the left ventricular posterior branch (short arrow).
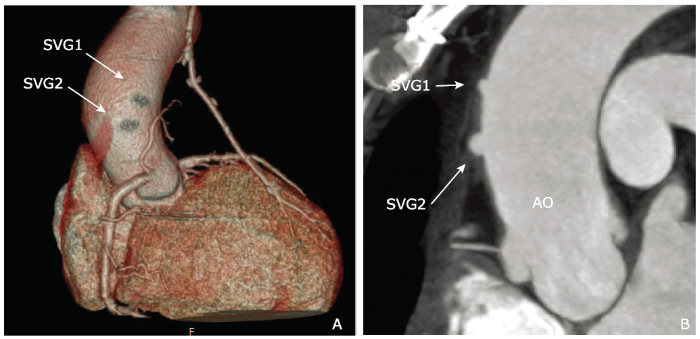
Figure 2.
MPR image and VR image of a 54-year-old male who had coronary artery bypass graft operation 15 months ago. VR image (A) and MPR image (B) show the two saphenous vein grafts (white arrows) were all occluded. SVG: saphenous vein graft; AO: aorta.
The MDCT examination revealed that, of 564 SV graft, 457 were patent (81.03%) (Fig. 1), and 107 were poor patent (Fig. 2). The patency rates of SV graft that were anastomosed to the diagonal branch(D), the obtuse marginal(OM) branch and the right coronary artery(RCA) were 69%(69/100), 85%(193/226) and 82%(195/238), respectively. The distribution of patency rates among all the territories of target vessels were statistically different (χ2=15.471,P=0.004) (Table 2).
Table 2 Distribution of LIMA and SV grafts patency among anastomosed vessels/territories of CABG
| Graft type | Target vessel | Patent, n (%) (n=751) | Poor patent, n (%) (n=143) | In total (n=894) |
|---|---|---|---|---|
| LIMA* | 294(89.1) | 36(10.9) | 330 | |
| LAD | 292(89.6) | 34(10.4) | 326 | |
| RCA | 2(50.0) | 2(50.0) | 4 | |
| SV** | 457(81.0) | 107(19.0) | 564 | |
| D | 69(69.0) | 31(31.0) | 100 | |
| OM | 193(85.4) | 33(14.6) | 226 | |
| RCA territory | 195(81.9) | 43(18.1) | 238 | |
*statistical analysis was not applicable; **chi-square test: X2=15.471, P=0.004.
LIMA:left internal mammary artery; SV:saphenous venous; LAD:left anterior descending branch; RCA:right coronary artery; D:diagonal branch; OM:obtuse marginal branch; RCA:right coronary artery.
Risk factors affecting patency of LIMA and SV grafts
Independent-samples t-test showed that the mean ages of patients with patent graft and poor patent graft were not significantly different for neither LIMA grafts (62.6±10.1 vs. 63.4±10.3 years, t=-0.45, P=0.65), nor SV grafts (62.8±10.1 vs. 62.4±10.3 years, t=-0.39, P=0.70). Univariates analysis for LIMA and SV graft patency (Table 3) showed that the gender, history of cerebrovascular disease, as well as luminal stenosis of proximal target vessel exceeding 90% were significantly associated to LIMA patency; the history of diabetes, hypertension, being symptomatic, and dyslipidemia were significantly associated to SV graft patency. Multivariate logistic regression analysis of graft patency showed the luminal stenosis of proximal target vessel of less than 90% was the independent risk factor for LIMA closure (OR=0.015, 95% CI: 0.01-0.14, P=0.000), and the history of diabetes, dyslipidemia, and being symptomatic were the independent risk factors for SV grafts closure (Table 4).
Table 3 Univariate analysis of factors that related to patency of LIMA grafts and SV grafts
| Variates | Patency of LIMA grafts | Patency of SV grafts | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Patent n=294 | Poor patent, n=36 | χ2 | P value | Patent n=457 | Poor patent n=107 | χ2 | Pvalue | ||
| Male, n (%) | 266(90.5) | 29(80.6) | 6.85 | 0.03 | 372(81.4) | 82(76.6) | 1.22 | 0.27 | |
| Hypertension, n(%) | 259(88.1) | 33(91.7) | 0.68 | 0.71 | 383(83.8) | 79(73.8) | 8.06 | 0.005 | |
| Dyslipidemia, n(%) | 259(88.1) | 32(88.9) | 2.53 | 0.28 | 340(74.4) | 91(85.0) | 3.56 | 0.04 | |
| Diabetes, n (%) | 267(90.8) | 32(88.9) | 1.08 | 0.58 | 345(75.5) | 89(83.2) | 4.39 | 0.036 | |
| Smoking, n (%) | 268(91.2) | 31(86.1) | 2.76 | 0.25 | 376(82.3) | 84(78.5) | 1.36 | 0.24 | |
| Cerebrovascular disease, n (%) | 230(78.2) | 33(91.7) | 10.47 | 0.005 | 366(80.1) | 86(80.4) | 0.00 | 0.98 | |
| Symptomatic, n(%) | 255(86.7) | 32(88.9) | 0.57 | 0.75 | 326(71.3) | 88(82.2) | 5.18 | 0.023 | |
| Proximal target vessel stenosis >90%, n (%) | 290(98.6) | 14(38.9) | 169 | <0.001 | NA | NA | NA | NA | |
NA:not applicable.
Table 4 Logistic regression analysis for the closure risk of LIMA grafts and SV grafts
| Risk factors | LIMA graft closure (n=330) | SV graft closure (n=564) | |||
|---|---|---|---|---|---|
| Odds ratio (95% CI) | Pvalue | Odds ratio (95% CI) | Pvalue | ||
| Gender | 3.82(0.73-20.05) | 0.11 | 1.38 (0.77-2.50) | 0.28 | |
| Hypertension | 1.99(0.39-10.05) | 0.41 | 0.61(0.38-0.98) | 0.04 | |
| Dyslipidemia | 1.48 (0.30-7.37) | 0.64 | 1.52(1.00-2.5) | 0.048 | |
| Diabetes | 0.14(0.02-1.32) | 0.09 | 1.28(0.90-2.26) | 0.045 | |
| Smoking | 0.53(0.10-2.93) | 0.47 | 0.96(0.59-1.57) | 0.88 | |
| Cerebrovascular disease | 2.55(0.41-15.93) | 0.32 | 1.0(0.53-1.88) | 1.00 | |
| Symptomatic | 1.01(0.09-11.25) | 0.99 | 1.81(1.33-4.15) | 0.003 | |
| Proximal target vessel stenosis <90% | 0.015(0.01-0.14) | 0.000 | NA | NA | |
DISCUSSION
In this study we used 64-MDCT to follow up the midterm outcomes of CABG. There were three major findings: firstly, the patency rate of CABG was higher in SV graft that was anastomosed to the OM or to RCA territory than that to the diagonal branch; secondly, the closure risk of LIMA graft was relatively high in patients whose luminal stenosis of proximal target vessel was less than 90%; thirdly, the occlusive risks of SV graft graft were relatively high in patients with history of dyslipidemia, diabetes, as well as those postoperatively experiencing typical anginal symptoms such as chest pain or dyspnea.
The impact of distant anastomosis site of bypass graft on its patency has rarely been reported in the literature. A previous study reported that the grafts anastomosed to LAD had better patency than those to RCA, 9 but subgroup analysis to delineate the ideal usage of each graft type wasn’t carried out. In this study, we delineated the graft type that was anastomosed to LAD territory, LCX territory and RCA territory, and found that the SVGs conduit to the LCX and RCA territory showed a significantly better patency than those to the D. This finding implied that the selection of the target anastomosis sites may influence on the graft patency. Histologically, the D has a smaller diameter of vessel than OM, RCA, PDA and PLB, therefore the mismatch of graft-target vessels size might account for the low patency rate of the SV graft anastomosed to the D.
Our study showed that the proximal LAD target vessel stenosis of less than 90% was adversely associated with LIMA patency. Otherwise, flow competition from native vessel would result in LIMA graft failure. This was consistent with previous study findings that the poor patency of LIMA graft might be caused by the vessels spasm or flow competition.14
It was believed that the failure of SV graft was caused by thrombosis, intimal hyperplasia or graft atherosclerosis.13, 15 Thrombosis mainly accounts for the graft failure in the first month after CABG, while intimal hyperplasia and graft atherosclerosis were regarded to associate with the delayed graft failure.16
This study found that suffering from type 2 diabetes, dyslipidemia, and being symptomatic of CHD yielded significant higher failure rate for SV graft, but not for LIMA graft. Yanagawa B et al 10 and Singh SK et al 11 also suggested that diabetes had significant impact on the SV graft failure. When comparing the study for radial arteries between the patients with diabetes and non-diabetic patients, there was no significant difference.11 Noyez L regarded that dyslipidemia and diabetes could promote the progress of atherosclerosis in the graft vessel, which is one of the main reasons for SV graft failure.16 We also found that symptomatic patients after SV graft operation had lower patency rate than those without symptom. This result is consistent with the findings in the study of Harskamp et al, where acute SV graft closure was found to lead to adverse coronary events, whereas slow-onset of SV graft failure did not. This is possibly because the developed collateral circulations take over the blood supplying. 17 Interestingly, we found that hypertension for patients who had SV graft might be a protective factor against its occlusion.
Our study showed female, history of cerebrovascular disease was associated with an increased risk of LIMA graft failure. In this study, the mean diameter of patent LIMA in female patients was shown to be less than that in male patients. Vessels with small diameter are not amendable to complete surgical revascularization, which may contribute to the grafts failure of LIMA in female. The history of cerebral vascular disease was shown to be a risk factor for graft failure in this study. Since cerebrovascular disease is usually associated with atherosclerosis, patients with cerebrovascular disease may have diffuse small-vessel coronary disease, which is not amendable to complete surgical revascularization and thus cause grafts failure.
There are several limitations in this study. Firstly, due to the experience and the preference of surgeons in our hospital, the number of patients with LIMA graft anastomosed to RCA was too small to perform statistical analysis. Secondly, as this is a retrospective observational study, the diameters of target vessels and the grafts could not be re-evaluated accurately. Thirdly, since 64-MDCT has been applied as routine to evaluate graft patency in our hospital for its well-recognized high accuracy,18 coronary angiography was not obtainable to double-confirm the MDCT observation in this study.
In conclusion, this retrospective study investigated patients of CABG who underwent midterm follow-up for the assessment of graft patency using 64-sclice MDCT. It is concluded that the proximal LAD target vessel stenosis of less than 90% was adversely associated with LIMA graft patency; type 2 diabetes, dyslipidemia, being anginal symptomatic were associated with the midterm failure of SV grafts, and selecting the target vessels for anastomosis may affect the patency of SV graft.
参考文献
Risk factors and in-hospital mortality in Chinese patients undergoing coronary artery bypass grafting: analysis of a large multi-institutional Chinese database

Author information: (1)Department of Cardiovascular Surgery, Children's National Heart Institute, Children's National Medical Center, Washington, DC 20010, USA. can.yerebakan@med.uni-rostock.de
Coronary vein graft disease: pathogenesis and prevention
Not long after coronary artery bypass grafting surgery was described, several reports presented follow-up angiographic data on large cohorts of patients, demonstrating that approximately one-half of saphenous vein grafts fail within 10 to 15 years of surgery and that graft failure is associated with worse clinical outcomes. Three processes are responsible for vein graft failure. Thrombosis, intimal hyperplasia and accelerated atherosclerosis contribute to graft failure in the acute, subacute and late postoperative periods, respectively. Studies have shown that perioperative antiplatelet therapy can reduce early thrombosis and graft failure. As in native coronaries, intensive lipid lowering can attenuate the process of atherosclerosis in vein grafts. Intimal hyperplasia in the vein graft is thought to be an adaptation of the vein to higher pressures in the arterial circulation. This process is further promoted by the loss of inhibition from the endothelial layer, which is injured during surgery. A new 鈥榥o-touch鈥 technique for harvesting grafts may be effective in preventing disruption to the endothelial layer, and subsequent intimal hyperplasia and graft loss. Off-pump surgery and endoscopic vein harvesting, which are known to reduce surgical morbidity, have been shown to be no worse than on-pump surgery and open vein harvesting, respectively, in terms of vein graft patency. Various gene therapies can prevent intimal hyperplasia in animal models, but human data obtained so far have been disappointing. Placing an external stent around a vein graft may reduce tangential wall stress and subsequent intimal hyperplasia.
Non-invasive coronary angiography: the clinical value of multi-slice computed tomography in the assessment of patients with prior coronary bypass surgery
Background Contrast enhanced multi-slice computed tomography (MSCT) is the leading modality in non-invasive coronary angiography (CTA) today. We investigated MSCT based assessment of coronary artery bypass grafts ( CABG ) by analyzing assets and drawbacks of CTA in order to define demands on latest technology. Methods In a clinical setting 39 CABG patients (69.202±021.402years; male n 02=0236) underwent CTA (collimation 1602×020.7502mm, contrast medium 10002ml; 32002mAs, 12002KV). Ninety-seven CABG (61 venous, 36 arterial grafts) were evaluated. A subgroup of 18 patients underwent additional invasive coronary angiography (CA). Results CTA for CABG assessment resulted in an overall sensitivity (sens.) of 100%, specificity (spec.) of 92.4% and positive and negative predictive values (PPV, NPV) of 60% and 100%, respectively. CABG anastomoses showed slightly inferior diagnostic accuracy than other CABG segments. Limitations in imaging quality caused 21% unevaluable segments of the CABG anastomoses. Evaluation of native vessel segments proximal and distal to the anastomoses resulted in a sens, spec, PPV and NPV of 57.5, 94.6, 92 and 67.3%, respectively. With 28.5% unevaluable segments, the native vessel segments showed serious limitations in imaging quality. Radiation exposure was 9.8802±023.2002mSv (9.6902±023.2502mSv male; 12.0802±021.3502mSv female). Conclusion 16-slice MSCT based CABG assessment offers sufficient diagnostic accuracy. However, focussing on the bypass anastomoses and the native revascularized coronary arteries, clinical value is limited.
CT angio for the evaluation of graft patency
Abstract Invasive coronary angiography (ICA) is the traditional method for the follow-up of graft patency in coronary artery bypass graft (CABG) patients. Nevertheless, the advent of multidetector computed tomography (MDCT) opened new perspectives for using a noninvasive, equally reliable method to study CABG patients. This review article will analyze the current feasibility of modern multi-slice MDCT, as well as its future perspectives.
Follow-up of coronary artery bypass graft patency: diagnostic efficiency of high-pitch dual-source 256-slice MDCT findings
Diagnostic accuracy and effective radiation dose of high pitch dual source multidetector computed tomography in evaluation of coronary artery bypass graft patency
Abstract Objective The aim of the study was to evaluate the diagnostic accuracy and effective radiation dose (ERD) of high pitch dual source multidetector computed tomography (MDCT) for coronary artery bypass graft (CABG) patency. Materials and methods Fourty-five patients who underwent 128 × 262slice MDCT angiography with a prospective electrocardiogram-triggering, low-dose, high pitch, dual source, flash spiral acquisition mode after CABG surgery were included in the study. The interobserver agreement of the image quality was evaluated with Cohen κ value. The image quality was compared to the heart rates (HRs) using Mann–Whitney U test and to the graft segments using χ2 test. The findings for the CABG patency on MDCT were compared to those determined on catheter coronary angiography. Dose-length product (DLP) and ERD were compared to the gender, HRs, and body mass index (BMI) of the patients using Kruskall Wallis and Mann–Whitney U tests. Results A total of 110 grafts and 330 vessel segments were evaluated with a good interobserver agreement (κ = 0.80). The image quality was better in proximal and middle graft segments (p < 0.05), as well as in the patients with low HRs (p < 0.05). High pitch MDCT had the following sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy for evaluation of graft patency: 92.8, 99.3, 92.8, 99.3 and 98.8 %, respectively. ERD was correlated to the HRs and BMI. Conclusions High pitch 128 × 262slice dual source CT angiography is a noninvasive imaging modality, and it can be safely and effectively used in evaluation of CABG patency with lower radiation dose.
Diagnostic accuracy of multidetector computed tomography coronary angiography in 325 consecutive patients referred for transcatheter aortic valve replacement
Multidetector computed tomography (MDCT) provides detailed assessment of valve annulus and iliofemoral vessels in transcatheter aortic valve replacement (TAVR) patients. However, data on diagnostic performance of MDCT coronary angiography (MDCT-CA) are scarce. The aim of the study is to assess diagnostic performance of MDCT for coronary artery evaluation before TAVR. A total of 325 consecutive patients (234 without previous myocardial revascularization, 49 with previous coronary stenting, and 42 with previous coronary artery bypass graft [CABG]) underwent invasive coronary angiography and MDCT before TAVR. MDCT-CA was performed using the same data set dedicated to standard MDCT aortic annulus evaluation. Multidetector computed tomography-CA evaluability and diagnostic accuracy in comparison with invasive coronary angiography as criterion standard were assessed. The MDCT-CA evaluability of native coronaries was 95.6%. The leading cause of unevaluability was beam-hardening artifact due to coronary calcifications. In a segment-based analysis, MDCT-CA showed sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy for detecting 50% stenosis of 91%, 99.2%, 83.4%, 99.6% and 98.8%, respectively. The MDCT-CA evaluability of coronary stents was 82.1%. In a segment-based analysis, MDCT-CA showed sensitivity, specificity, PPV, NPV, and accuracy for detecting 鈮50% in-stent restenosis of 94.1%, 86.7%, 66.7%, 98.1%, and 88.3%, respectively. All CABGs were correctly assessed by MDCT-CA. In a patient-based analysis, MDCT-CA showed sensitivity, specificity, PPV, NPV, and accuracy of 89.7%, 90.8%, 80.6%, 95.4%, and 90.5%, respectively. Multidetector computed tomography A allows to correctly rule out the presence of significant native coronary artery stenosis, significant in-stent restenosis, and CABG disease in patients referred for TAVR.
Comparison of multidetector 64-slice computed tomographic angiography to coronary angiography to assess the patency of coronary artery bypass grafts
This study prospectively evaluated the diagnostic accuracy of 64-slice computed tomographic angiography (CTA) in assessing the patency of coronary artery bypass grafts compared with invasive coronary angiography. In total 147 bypass grafts (100 venous grafts and 47 mammary artery grafts) were evaluated in 50 consecutive patients. Contrast-enhanced 64-slice CTA was performed and compared with invasive angiography. The computed tomographic angiographic scan protocol used 64- 0.5-mm slice collimation and 0.33-second gantry rotation time during simultaneous electrocardiographic gating. Patients with a heart rate >65 beats/min received blockers. Overall 145 of 147 bypass grafts (98.6%) were detected by CTA; 2 nonvisualized grafts were occluded at the time of invasive angiography. Of the grafts visualized, 28 were totally occluded, 103 were patent, and 14 had significant stenoses that were confirmed by invasive angiography. Ninety-five percent (111 of 117) of patent grafts demonstrated good run-off distal to anastomoses but without an ability to accurately evaluate the presence of retrograde flow; 83% (97 of 117) of distal anastomoses were adequately evaluated, whereas the remaining 17% (20 of 117) were not well visualized due to vascular clips and/or calcification artifacts. Two grafts were not demonstrated by invasive angiography but were detected by CTA and found to be widely patent. In conclusion, multidetector 64-slice CTA is a valuable tool for direct visualization of coronary bypass grafts and assessment of their patency. Dysfunctional bypass grafts can be detected with high diagnostic accuracy.
Karlsberg, RP. Long-term coronary artery graft patency as evaluated by 64-slice coronary computed tomographic angiography
Coronary artery bypass graft (CABG) surgery has been a mainstream surgical procedure for coronary artery disease for the past three decades. 64-Slice coronary computed tomographic angiography (CCTA) has been established as an accurate alternative to invasive coronary artery angiography for postoperative evaluation of bypass grafts. The goal for this study was to utilize CCTA to evaluate long-term graft patency for various graft types as well as their targets.We analyzed all consecutive patients with a history of coronary artery bypass graft undergoing CCTA over a 3-year period. A total of 827 grafts in 269 patients were included in the study.Mean survival of the grafts was 21 years (95% confidence interval 20.6, 22.3). The mean survival of grafts to the left anterior descending coronary artery, the left circumflex coronary artery, and the right coronary artery were 22.9, 20.6, and 20.1 years, respectively (P=0.05). Evaluation of graft types demonstrated internal thoracic artery grafts, saphenous venous grafts, and radial artery grafts (RA) had a mean survival of 20.5 years, 21.6 years, and 12.6 years, respectively (P=0.05). Factors significantly affecting the time to closure (P 0.01) were age [odds ratio (OR) 1.03], male sex (OR 2.39), smoking (OR 2.07), left anterior descending coronary artery graft territory (OR 0.55 compared with right coronary artery), and RA (OR 3.65 compared with thoracic artery grafts, 3.79 compared with saphenous venous grafts).In conclusion, this study confirms the practicality of using CCTA in a community setting to study bypass graft patency. The choice of graft is significant for long-term patency. This study raises doubt on the long-term fate of RA and further studies should be conducted to better evaluate their outcomes.
Clinical, biochemical, genetic predictors of coronary artery bypass graft failure
To identify novel predictors for coronary artery bypass grafting failure, we probed for associations with known clinical and biochemical risk factors for atherosclerosis. We also used microarray analysis to identify novel single nucleotide polymorphisms to better understand the genetics and pathogenesis of graft occlusion. The present study was a nested case-control substudy of the Radial Artery Patency Study 5-year follow-up data. From 1996 to 2001, 87 patients underwent coronary artery bypass grafting. Of these, 26 patients (29.9%) had an occluded study graft (saphenous vein or radial artery) at 8.0 ± 1.1 years. The clinical parameters, late angiography, blood biomarker levels, and surgical outcomes data were included in a multivariate analysis to determine the independent predictors of graft failure. The risk factors of graft failure were fibrinogen (odds ratio [OR], 3.94; 95% confidence interval [CI], 1.33-11.63; P02=02.01), creatinine (OR, 1.06; 95% CI, 1.02-1.10; P02=02.006), and diabetes mellitus (OR, 5.15; 95% CI, 1.08-24.59; P02=02.04). High-density lipoprotein (OR, 0.74; 95% CI, 0.53-1.02; P02=02.06) was weakly protective; however, low-density lipoprotein and total cholesterol were not predictors. We then identified the association of several human single nucleotide polymorphisms with graft failure, including mutations in glutathione-S-transferase α3. Human coronary arteries and bypass grafts demonstrated increased protein expression of glutathione-S-transferase α3, a known cardioprotective factor, in the atherosclerotic regions and surrounding adventitial tissues. We identified diabetes as a potential clinical predictor and plasma fibrinogen, creatinine, and high-density lipoprotein as potential novel biomarkers. These might help risk stratify patients for the development of graft failure. We also demonstrated a novel association between glutathione-S-transferase α3 and graft failure.
The impact of diabetic status on coronary artery bypass graft patency: insights from the radial artery patency study
BACKGROUND: Despite worse outcomes in diabetics after coronary artery bypass grafting surgery, studies have not examined graft patency in this high-risk group. This study examined the impact of diabetes on graft patency, 1-year postcoronary artery bypass grafting, using data from a multicenter randomized trial. METHODS AND RESULTS: The Radial Artery Patency Study enrolled 561 patients undergoing coronary artery bypass grafting, comparing graft patency of the saphenous vein (SV) versus radial artery 1-year postcoronary artery bypass grafting. Angiographic follow-up was acquired for 440 patients (115 diabetics, 325 nondiabetics), each with a study radial artery and a control SV graft. Preoperative characteristics were similar. The proportion of small-sized target vessels was greater in diabetics (P=0.04). At 1 year, 33 of 230 study grafts (14.4%) were occluded in the diabetics versus 63 of 650 (9.7%) in the nondiabetics (P=0.052). Multivariable regression found diabetes to be a significant independent predictor of 1-year graft occlusion (relative risk, 1.45; 95% CI, 1.03 to 2.05; P=0.03) along with female gender, SV conduit, and small target-vessel size. A significantly higher proportion of SV grafts were occluded in the diabetics (19% versus 12%, P=0.04). Radial artery grafting was protective in the diabetic cohort (radial artery: 11 of 115 occluded [9.5%] versus SV: 22 of 115 occluded [19.1%], McNemar corrected P=0.05; relative risk, 0.42; 95% CI, 0.16 to 1.01) and nondiabetics (radial artery: 25 of 325 occluded [7.7%] versus SV: 38 of 325 occluded [11.7%], McNemar corrected P=0.11; relative risk, 0.63; 95% CI, 0.35 to 1.10). CONCLUSIONS: Coronary artery bypass grafting occlusions were more common among diabetics versus nondiabetics at 1-year angiography, mainly because of more frequent SV graft failure in diabetics. Radial artery, compared with SV grafting, is protective in both diabetic and nondiabetic patients.
Does diabetes affect the postoperative outcomes after total arterial off-pump coronary bypass surgery in multivessel disease?
Previous studies have reported conflicting results regarding the adverse effects of diabetes on surgical outcomes after coronary artery bypass grafting (CABG). We reviewed our experience to determine the impact of diabetes on early and midterm surgical outcomes of patients with multivessel disease who underwent total arterial revascularization with avoidance of cardiopulmonary bypass. Between January 1998 and December 2003, 517 patients with multivessel disease underwent total arterial off-pump CABG; 214 were diabetic (DM group) and 303 were nondiabetic (NDM group). The DM group was sicker than the NDM group (more left ventricular dysfunction, postinfarction angina, previous myocardial infarction, and chronic renal failure). Mean follow-up period was 34 17 months. The multivariate risk factors for operative mortality, one-year angiographic patency, and midterm survival were analyzed. Mean numbers of distal anastomoses were not different between the two groups (DM, 3.1 0.9; NDM, 3.0 0.8). Operative mortality was 1.4% (DM, 1.4% vs NDM, 1.3%; p = not significant [ns]). No differences were found in the incidences of postoperative morbidities, including mediastinitis and superficial wound problems, between the two groups. In immediate postoperative angiography, the patency rates were 99.2% in the DM and 98.9% in the NDM group ( p = ns). One-year patency rates in angiography were also similar between the two groups (DM, 96.0%; NDM, 95.4%; p = ns). Multivariate analysis indicated that diabetes was not an independent risk factor of steno-occlusion at one-year follow-up angiography. Five-year cumulative survival was 87.7 4.1% in the DM, and 94.2 1.4% in NDM ( p = ns) group. Five-year freedom from cardiac death was 99.0 0.7% in the DM, and 97.4 1.0% in the NDM ( p = ns) group. Old age (age >75 years) and chronic renal failure were independent risk factors for lower midterm survival. Our study failed to demonstrate that diabetes was an independent risk factor for lower midterm survival. Diabetes mellitus did not affect the early postoperative and midterm results, including one-year graft patency, in patients with multivessel disease undergoing total arterial and off-pump CABG.
Coronary bypass graft fate and patient outcome: angiographic follow-up of 5065 grafts related to survival and reoperation in 1388 patients during 25 years
Late improvement in graft patency after coronary artery bypass grafting: serial assessment with multidetector computed tomography in the early and late postoperative settings
Grafts initially showing poor patency after coronary artery bypass grafting have occasionally shown improvement on serial multidetector computed tomography. This study analyzed possible factors associated with this phenomenon. Between September 2003 and July 2007, 512 patients underwent multidetector computed tomography within 1 month of isolated coronary artery bypass grafting. Among them, 1720 distal anastomoses were made with 1042 arterial and 302 venous conduits. Of these, 95 grafts (in 73 patients) were faint (n02=0267) or nonvisualized (n02=0228). Seventy-three of these grafts (in 56 patients) had follow-up multidetector computed tomographic evaluation 1 year after surgery and comprised the study group. Improvement in graft patency (faint to patent or nonvisualization to visualization) occurred in 44 grafts (60.3%). Multivariate analysis revealed proximal target vessel stenosis of at least 90% (relative risk, 3.81; P02=02.009), larger target coronary size (relative risk, 1.72; P02=02.002), and radial artery graft use (relative risk, 4.44; P02=02.003) to be significantly associated with the graft patency restoration. Graft patency restoration was most commonly observed in a group of 28 radial artery grafts that were anastomosed to target vessel with proximal stenosis of at least 90%; of these grafts, 24 (85.7%) showed improved graft patency on follow-up. A large proportion of radial artery grafts initially showing poor opacification after coronary artery bypass grafting demonstrated patency restoration on serial multidetector computed tomography. Larger target vessel size and target vessel stenosis of at least 90% were significant correlative factors.
Coronary artery bypass graft disease
Abstract PURPOSE: To review saphenous vein graft disease and its prevention and management. DATA SOURCES: A MEDLINE search of articles published on saphenous vein and arterial bypass grafts. STUDY SELECTION: The reference sections of articles focused the selection of key studies. DATA EXTRACTION: Relevant data representing key findings were noted. DATA SYNTHESIS: The outcome of coronary artery bypass grafting with the saphenous vein graft is unsatisfactory because vein grafts are prone to occlusive disease. By 10 years after surgery, 50% have closed, mainly because of atherosclerosis. With vein graft disease and graft closure, symptoms return. The best way to prevent vein graft disease is to use the internal mammary artery graft. This has become the preferred graft because it is not affected by atherosclerosis. Consequently, it has a much higher patency rate: 90% after more than 10 years. This provides such clinical benefits as decreased occurrence of symptoms, better left ventricular performance, decreased need for reoperation, and prolongation of life. The limited supply of mammary arteries has stimulated interest in identifying alternative arterial grafts. CONCLUSIONS: To prevent vein graft disease, surgeons should bypass diseased coronary arteries with at least one arterial graft and take measures during the surgery to avoid endothelial injury to vein grafts. Treatment with antiplatelet agents decreases the vein graft occlusion rate. When graft atherosclerosis causes symptoms, reoperation will probably prolong life if an old graft to the left anterior descending coronary artery is diseased. Reoperation increases a patient's chance for survival if the surgeon uses at least one arterial graft.
The evolution of repeat coronary artery surgery
Abstract As has been seen in primary coronary artery bypass surgery (CABG), the patient population undergoing surgical secondary revascularisation (RECABG) has changed during the last twenty years. An increasing number of older patients, with more coexisting disease, are presented for RECABG. Beside the demographic changes, there are also changes as a part of the results of the different strategies used in CABG. The extensive use of arterial grafts in CABG results in an increase of the event-free period and of the period between CABG and RECABG. But results also show a challenge for RECABG with a patent arterial graft. Also, routine use of antiplatelet drugs and statins after CABG have an influence on the patient population presented for secondary revascularisation. Probably the most important aspect here is the evolution in percutaneous coronary intervention (PCI), especially in combination with a patent arterial graft protecting part of the myocardium. The purpose of this paper is to review the evolutionary trends in the patient population undergoing secondary revascularisation.
Saphenous vein graft failure and clinical outcomes: toward a surrogate end point in patients following coronary artery bypass surgery?
Saphenous vein graft (SVG) failure is a common finding in patients following coronary artery bypass graft (CABG) surgery. In the literature SVG failure rates have been reported from 25 to over 50% within 10 years. Although common, it remains unclear to what extent SVG failure affects clinical outcome, due to differences in definition, patient selection and follow-up. Particularly the lack of agreement on a universal definition makes comparisons between studies, and therefore generalizability of associations with outcomes, challenging. We suggest using a definition of SVG failure that is based on imaging as well as clinical parameters, that includes reporting SVG failure on both graft and patient level. The use of non-invasive imaging may help improve follow-up rates, and provide a more accurate picture of the real incidence and clinical impact of SVG failure. Given the lack of supportive evidence showing a consistent association between SVG failure and major adverse cardiovascular events, SVG failure should not be considered a valid surrogate endpoint at this time.
A systematic review and meta-analysis of multidetector computed tomography in the assessment of coronary artery bypass grafts
61Assessment of combined stenosis or occlusion has a high pooled sensitivity and specificity.61CTCA assessment of venous grafts demonstrated higher sensitivity compared to arterial grafts.61CTCA is an accurate and non-invasive investigation for graft patency in symptomatic patients after CABG.

{kind=link}
{kind=link}
{kind=link}
{kind=link}