Chinese Medical Sciences Journal ›› 2021, Vol. 36 ›› Issue (1): 17-26.doi: 10.24920/003866
高脂血症与新型冠状病毒肺炎住院患者28天全因死亡率的关系
吴斌1,周江华1,2,汪文鑫1,2,杨慧琳2,3,夏盟2,张丙宏4,折志刚1,2,李红良1,2,3,5,*( )
)
- 1武汉大学人民医院心内科,武汉430071,中国
2武汉大学模式动物研究所,武汉430071,中国
3武汉大学基础医学院,武汉430071,中国
4武汉大学人民医院新生儿科,武汉430072,中国
5武汉大学中南医院,医学科学研究中心,武汉430071,中国
-
收稿日期:2021-02-09接受日期:2021-03-05出版日期:2021-03-17发布日期:2021-03-17 -
通讯作者:李红良 E-mail:lihl@whu.edu.cn
Association Analysis of Hyperlipidemia with the 28-Day All-Cause Mortality of COVID-19 in Hospitalized Patients
Bin Wu1,Jianghua Zhou1,2,Wenxin Wang1,2,Huilin Yang2,3,Meng Xia2,Binghong Zhang4,Zhigang She1,2,Hongliang Li1,2,3,5,*()
- 1Department of Cardiology, Renmin Hospital of Wuhan University, Wuhan 430071, China
2Institute of Model Animal, Wuhan University, Wuhan 430071, China
3Basic Medical School, Wuhan University, Wuhan 430071, China
4Department of Neonatology, Renmin Hospital of Wuhan University, Wuhan 430072, China
5Medical Science Research Center, Zhongnan Hospital of Wuhan University, Wuhan 430071, China
-
Received:2021-02-09Accepted:2021-03-05Published:2021-03-17Online:2021-03-17 -
Contact:Hongliang Li E-mail:lihl@whu.edu.cn
摘要:
目的 本研究旨在确定高脂血症与COVID-19住院患者的临床终点之间的关联,尤其是那些伴随心血管疾病(cardiovascular diseases, CVDs)和糖尿病的COVID-19患者。
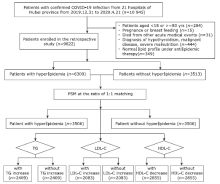
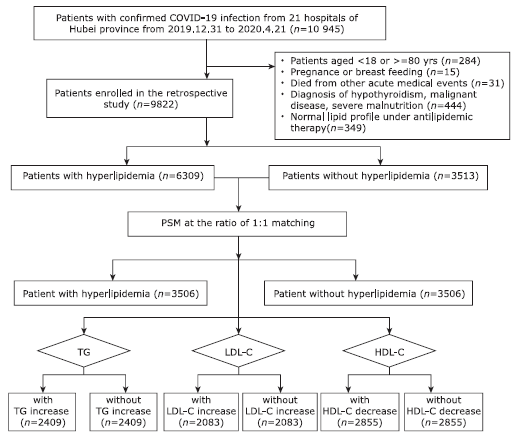
方法 这项多中心回顾性队列研究搜集2019年12月31日至2020年4月21日期间中国湖北省21家医院全部确诊COVID-19的住院患者。 我们排除了年龄<18岁或≥85岁、处于妊娠期间、患有急性致死性器官损伤(如急性心肌梗塞,严重的急性胰腺炎或急性中风)、甲状腺功能减退、恶性疾病、严重的营养不良以及因服用降脂药物(如他汀类,烟酸,非诺贝特或吉非贝齐,依泽替米贝)而血脂正常的患者。采用1:1倾向性评分匹配(Propensity score matching,PSM)控制高脂血症组和非高脂血症组的患者的基线特征差异,并以相同的PSM策略对不同高脂血症参数亚组进行匹配, 包括甘油三酸酯(triglyceride,TG)升高组,低密度脂蛋白胆固醇(low-density lipoprotein cholesterol, LDL-C)升高组和高密度脂蛋白胆固醇(high-density lipoprotein cholesterol, HDL-C)降低组。采取混合效应Cox模型分析总体以及各亚组内高脂血症与COVID-19患者28天全因死亡率之间的相关性,并分别在男性、女性、伴有CVDs及伴有2型糖尿病患者的亚组中对结果进行验证分析。
结果 在10 945例住院的COVID-19患者中,共9822例纳入研究,包括6309例(64.2%)血脂升高患者和3513例(35.8%)血脂正常患者。按1:1的倾向性评分匹配后经混合效应Cox模型分析显示,与血脂正常组相比,高脂血症不显著增加或减少COVID-19患者28天全因死亡风险(HR=1.17, 95% CI,0.95~1.44, P=0.151)。COVID-19患者预后与血脂各参数异常亦无显著关联,包括TG升高(HR=1.23,95% CI,0.98~1.55,P=0.075),LDL-C升高(HR=0.78;95% CI,0.57~1.07,P=0.123),以及HDL-C降低(HR=1.12,95% CI,0.90~1.39,P=0.299)。在伴有心血管疾病、伴有糖尿病的COVID-19患者亚组中,以及在男性或女性COVID-19患者亚组中,高脂血症与COVID-19全因死亡率均无显著相关性。
结论 我们的研究表明,即使在伴有心血管疾病和伴有糖尿病的患者中,脂质分布失衡与COVID-19的28天全因死亡率也无显着相关性。分别对TG,HDL-C及LDL-C脂质参数的高脂血症亚组分析也获得了相似的结果。因此,脂质失衡可能不是导致与心血管代谢性疾病相关的COVID-19不良预后的主要原因。该结果为COVID-19流行期间住院患者的干预提供了参考。
引用本文
Bin Wu,Jianghua Zhou,Wenxin Wang,Huilin Yang,Meng Xia,Binghong Zhang,Zhigang She,Hongliang Li. Association Analysis of Hyperlipidemia with the 28-Day All-Cause Mortality of COVID-19 in Hospitalized Patients[J].Chinese Medical Sciences Journal, 2021, 36(1): 17-26.
"
"
| Characteristics | Study cohort | Cohort after matching (1:1)b | |||||
|---|---|---|---|---|---|---|---|
| Hyperlipidemia a (n=6309) | Normal (n=3513) | SD | Hyperlipidemia a (n=3506) | Normal (n=3506) | SD | ||
| Age [years, median (IQR)] | 59(48-68) | 59(45-68) | 0.083 | 58(47-67) | 59(45-68) | -0.001 | |
| Gender-male [n (%)] | 3387(53.69) | 1450(41.28) | 0.250 | 1597(45.55) | 1450(41.36) | 0.085 | |
| Heart rate [bpm, median (IQR)] | 85(78-97) | 84(78-96) | 0.049 | 85(78-96) | 84(78-96) | 0.005 | |
| Respiratory [bpm, median(IQR)] | 20(19-21) | 20(19-21) | 0.104 | 20(19-21) | 20(19-21) | -0.018 | |
| SBP [mmHg, median (IQR)] | 129(120-141) | 128(118-139) | 0.087 | 128(119-140) | 128(118-139) | 0.025 | |
| DBP [mmHg, median (IQR)] | 80(72-88) | 79(72-86) | 0.101 | 79(72-87) | 79(72-86) | 0.038 | |
| SpO2 [%, median(IQR)] | 97(95-98) | 97(96-98) | -0.06 | 98(96-98) | 97(96-98) | 0.024 | |
| Comorbidities on admission [n (%)] | |||||||
| Chronic obstructive pulmonary disease | 67(1.06) | 47(1.34) | -0.025 | 45(1.28) | 45(1.28) | 0.000 | |
| Diabetes | 1095(17.36) | 408(11.61) | 0.164 | 386(11.01) | 408(11.64) | -0.020 | |
| Heart failure | 40(0.63) | 23(0.65) | -0.003 | 20(0.57) | 23(0.66) | -0.011 | |
| Coronary heart disease | 603(9.56) | 195(5.55) | 0.152 | 204(5.82) | 195(5.56) | 0.011 | |
| Cerebrovascular diseases | 196(3.11) | 81(2.31) | 0.049 | 89(2.54) | 81(2.31) | 0.015 | |
| Chronic liver disease | 151(2.39) | 76(2.16) | 0.015 | 75(2.14) | 76(2.17) | -0.002 | |
| Chronic renal diseases | 266(4.22) | 103(2.93) | 0.002 | 112(3.19) | 103(2.94) | 0.015 | |
| Medications [n (%)] | |||||||
| Insulin | 975(15.45) | 320(9.11) | 0.194 | 332(9.47) | 320(9.13) | 0.012 | |
| Oral hypoglycemic drugs | 1352(21.43) | 456(12.98) | 0.225 | 474(13.52) | 456(13.01) | 0.015 | |
| non-ACEI/ARB antihypertensive drug | 1907(30.23) | 873(24.85) | 0.121 | 814(23.22) | 872(24.87) | -0.039 | |
| ACEI/ARB | 628(9.95) | 233(6.63) | 0.121 | 215(6.13) | 233(6.65) | -0.021 | |
| Antiplatelet | 533(8.45) | 110(3.13) | 0.229 | 89(2.54) | 110(3.14) | -0.036 | |
| Chest CT on admission [n (%)] | |||||||
| Bilateral lesions | 5154(87.05) | 2808(83.60) | 0.098 | 2718(83.35) | 2807(83.74) | -0.011 | |
| Lab tests on admission [n (%), or median(IQR)] | |||||||
| Leukocyte count > 9.5×109/L | 697(11.08) | 270(7.71) | 0.116 | 313(8.98) | 270(7.73) | 0.045 | |
| Neutrophil count > 6.3×109/L | 1062(16.89) | 412(11.77) | 0.146 | 455(13.05) | 412(11.80) | 0.038 | |
| Lymphocyte< 1.1×109/L | 2595(41.26) | 1400(40.00) | 0.026 | 1405(40.28) | 1394(39.91) | 0.008 | |
| RBC < 3.5×1012/L (female) or 4.0×1012/L (male) | 2568(40.83) | 1579(45.14) | -0.087 | 1441(41.32) | 1574(45.09) | -0.076 | |
| CRP > ULN c | 2103(52.65) | 821(46.10) | 0.131 | 1257(51.52) | 819(46.11) | 0.108 | |
| PCT > ULN c | 2479(45.06) | 1021(34.95) | 0.207 | 954(31.39) | 1020(34.99) | -0.076 | |
| ALT > 40 U/L | 1679(26.63) | 640(18.23) | 0.202 | 611(17.45) | 640(18.27) | -0.021 | |
| eGFR value (mL/min) | 103.57 (87.61-120.50) | 105.30 (89.21-122.61) | -0.073 | 107.34 (91.14-125.22) | 105.29 (89.21-122.55) | 0.043 | |
| D-dimer > ULN c | 3024(52.06) | 1351(42.26) | 0.197 | 1479(46.88) | 1351(42.32) | 0.092 | |
| cTnI > ULN c | 446(10.96) | 160(7.35) | 0.125 | 153(7.65) | 160(7.36) | 0.013 | |
"
| Categories | Number of patients (n) | Deaths (n) | Adjusted HR (95% CI) | P value a |
|---|---|---|---|---|
| All patients of matched cohort b | ||||
| Hyperlipidemia group vs. non-hyperlipidemia group | 3506 vs. 3506 | 231 vs. 193 | 1.17 (0.95, 1.44) | 0.151 |
| TG ≥1.7 mmol/L group vs. TG<1.7 mmol/L group | 2409 vs. 2409 | 180 vs. 137 | 1.23 (0.98, 1.55) | 0.075 |
| LDL-C ≥3 mmol/L group vs. LDL-C<3 mmol/L group | 2083 vs. 2083 | 67 vs. 95 | 0.78 (0.57, 1.07) | 0.123 |
| HDL-C <1.0 mmol/L group vs. HDL-C ≥1.0 mmol/L group | 2855 vs. 2855 | 213 vs. 157 | 1.12 (0.90, 1.39) | 0.299 |
| Male patients in matched cohort c | ||||
| Hyperlipidemia group vs. non-hyperlipidemia group | 1449 vs. 1449 | 135 vs. 112 | 1.24 (0.91, 1.70) | 0.176 |
| TG ≥1.7 mmol/L group vs. TG<1.7 mmol/L group | 1145 vs. 1145 | 114 vs. 81 | 1.23 (0.92, 1.66) | 0.170 |
| LDL-C ≥3 mmol/L group vs. LDL-C<3 mmol/L group | 988 vs. 988 | 43 vs. 46 | 1.00 (0.65, 1.52) | 0.983 |
| HDL-C <1.0 mmol/L group vs. HDL-C ≥1.0 mmol/L group | 1499 vs. 1499 | 131 vs. 86 | 1.27 (0.94, 1.72) | 0.113 |
| Female patients in matched cohort d | ||||
| Hyperlipidemia group vs. non-hyperlipidemia group | 2014 vs. 2014 | 92 vs. 81 | 0.91 (0.66, 1.25) | 0.547 |
| TG ≥1.7 mmol/L group vs. TG<1.7 mmol/L group | 1233 vs. 1233 | 62 vs. 50 | 1.14 (0.78, 1.66) | 0.509 |
| LDL-C ≥3 mmol/L group vs. LDL-C<3 mmol/L group | 1099 vs. 1099 | 24 vs. 33 | 0.82 (0.48, 1.39) | 0.456 |
| HDL-C <1.0 mmol/L group vs. HDL-C ≥1.0 mmol/L group | 1326 vs. 1326 | 79 vs. 66 | 1.00 (0.71, 1.40) | 0.993 |
"
| Categories | Number of Patients (n) | Deaths (n) | Adjusted HR (95% CI) | P value a |
|---|---|---|---|---|
| Cardiovascular diseases b | ||||
| Hyperlipidemia group vs. non-hyperlipidemia group | 1242 vs. 1242 | 128 vs. 114 | 0.96 (0.73,1.26) | 0.765 |
| TG ≥1.7 mmol/L group vs. TG<1.7 mmol/L group | 1004 vs. 1004 | 115 vs. 81 | 1.19 (0.88,1.60) | 0.253 |
| LDL-C ≥3 mmol/L group vs. LDL-C<3 mmol/L group | 814 vs. 814 | 42 vs. 59 | 0.78 (0.52,1.17) | 0.235 |
| HDL-C <1.0 mmol/L group vs. HDL-C ≥1.0 mmol/L group | 1131 vs. 1131 | 124 vs. 90 | 1.00 (0.75,1.33) | 0.991 |
| Type 2 diabetes c | ||||
| Hyperlipidemia group vs. non-hyperlipidemia group | 473 vs. 473 | 52 vs. 54 | 0.74 (0.49,1.13) | 0.164 |
| TG ≥1.7 mmol/L group vs. TG<1.7 mmol/L group | 515 vs. 515 | 56 vs. 40 | 1.07 (0.70,1.64) | 0.752 |
| LDL-C ≥3 mmol/L group vs. LDL-C<3 mmol/L group | 364 vs. 364 | 20 vs. 29 | 0.72 (0.40,1.30) | 0.279 |
| HDL-C <1.0 mmol/L group vs. HDL-C ≥1.0 mmol/L group | 492 vs. 492 | 56 vs. 43 | 1.17 (0.76,1.81) | 0.468 |
| 1. |
Zhang P, Zhu L, Cai J, et al. Association of inpatient use of angiotensin-converting enzyme inhibitors and angiotensin Ⅱ receptor blockers with mortality among patients with hypertension hospitalized with COVID-19. Circ Res 2020; 126(12):1671-81. doi: 10.1161/CIRCRESAHA.120.317134.
doi: 10.1161/CIRCRESAHA.120.317134 pmid: 32302265 |
| 2. |
Zhu L, She ZG, Cheng X, et al. Association of blood glucose control and outcomes in patients with COVID-19 and pre-existing type 2 diabetes. Cell Metab 2020;31(6):1068-77.e3. doi: 10.1016/j.cmet.2020.04.021.
doi: 10.1016/j.cmet.2020.04.021 pmid: 32369736 |
| 3. |
Guo T, Fan Y, Chen M, et al. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol 2020; 5(7):811-8. doi: 10.1001/jamacardio.2020.1017.
doi: 10.1001/jamacardio.2020.1017 pmid: 32219356 |
| 4. |
Bornstein SR, Rubino F, Khunti K, et al. Practical recommendations for the management of diabetes in patients with COVID-19. Lancet Diabetes Endocrinol 2020; 8(6):546-50. doi: 10.1016/S2213-8587(20)30152-2.
doi: 10.1016/S2213-8587(20)30152-2 pmid: 32334646 |
| 5. | Ni WQ, Liu XL, Zhuo ZP, et al. Serum lipids and associated factors of dyslipidemia in the adult population in Shenzhen. Lipids Health Dis 2015; 14(1):1-11. doi: 10.1186/s12944-015-0073-7. |
| 6. |
Palaiodimos L, Kokkinidis DG, Li W, et al. Severe obesity is associated with higher in-hospital mortality in a cohort of patients with COVID-19 in the Bronx, New York. Metabolism 2020; 108:154262. doi: 10.1016/j.metabol.2020.154262.
doi: 10.1016/j.metabol.2020.154262 pmid: 32422233 |
| 7. | Abu-Farha M, Thanaraj TA, Qaddoumi MG, et al. The role of lipid metabolism in COVID-19 virus infection and as a drug target. Int J Mol Sci 2020; 21(10):3544. doi: 10.3390/ijms21103544. |
| 8. |
Tanaka S, Labreuche J, Drumez E, et al. Low HDL levels in sepsis versus trauma patients in intensive care unit. Ann Intensive Care 2017; 7(1):4-11. doi: 10.1186/s13613-017-0284-3.
doi: 10.1186/s13613-016-0231-8 pmid: 28050897 |
| 9. | Peñarrubia L, Ruiz M, Porco R, et al. Multiple assays in a real-time RT-PCR SARS-CoV-2 panel can mitigate the risk of loss of sensitivity by new genomic variants during the COVID-19 outbreak. Int J Infect Dis 2020; 97:225-9. doi: 10.1016/j.ijid.2020.06.027. |
| 10. | Official website of the National Health Commission of People’s Republic of China. The prevention and control guideline for novel coronavirus pneumonia (5th edition). . |
| 11. | Joint committee issued Chinese guideline for the management of dyslipidemia. 2016 Chinese guideline for the management of dyslipidemia in adults. Zhonghua Xin Xue Guan Bing Za Zhi 2016; 44(10):833-53. Chinese. doi: 10.3760/cma.j.issn.0253-3758.2016.10.005. |
| 12. |
Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Atherosclerosis 2019; 290:140-205. doi: 10.1016/j.atherosclerosis.2019.08.014.
doi: 10.1016/j.atherosclerosis.2019.08.014 pmid: 31591002 |
| 13. | Chinese Diabetes Society; National Office for Primary Diabetes Care. National guidelines for the prevention and control of diabetes in primary care( 2018). Zhonghua nei ke za zhi 2018; 57(12):885-93. Chinese. doi: 10.3760/cma.j.issn.0578-1426.2018.12.003. |
| 14. | Jakubowski KP, Cundiff JM, Matthews KA. Cumulative childhood adversity and adult cardiometabolic disease: A meta-analysis. Heal Psychol 2018; 37(8):701-15. doi: 10.1037/hea0000637. |
| 15. | Tay MZ, Poh CM, Rénia L, et al. The trinity of COVID-19: immunity, inflammation and intervention. Nat Rev Immunol 2020; 20(6):363-74. doi: 10.1038/s41577-020-0311-8. |
| 16. |
Cao X. COVID-19: immunopathology and its implications for therapy. Nat Rev Immunol 2020; 20(5):269-70. doi: 10.1038/s41577-020-0308-3.
pmid: 32273594 |
| 17. | Touyz RM, Li H, Delles C. ACE2 the Janus-faced protein-from cardiovascular protection to severe acute respiratory syndrome-coronavirus and COVID-19. Clin Sci 2020; 134(7):747-50. doi: 10.1042/CS20200363. |
| 18. | Chen T, Wu D, Chen H, et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020; 368(m1091):1-14. doi: 10.1136/bmj.m1091. |
| 19. |
Richardson S, Hirsch JS, Narasimhan M, et al. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York city area. JAMA 2020; 323(20):2052-9. doi: 10.1001/jama.2020.6775.
pmid: 32320003 |
| 20. |
Shao B, Heinecke JW. HDL, lipid peroxidation, and atherosclerosis. J Lipid Res 2009; 50(4):599-601. doi: 10.1194/jlr.E900001-JLR200.
doi: 10.1194/jlr.E900001-JLR200 pmid: 19141435 |
| 21. |
Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med 2005; 352(16):1685-95. doi: 10.1056/NEJMra043430.
pmid: 15843671 |
| 22. |
Steinberg D. An interpretive history of the cholesterol controversy, part III: Mechanistically defining the role of hyperlipidemia. J Lipid Res 2005; 46(10):2037-51. doi: 10.1194/jlr.R500010-JLR200.
doi: 10.1194/jlr.R500010-JLR200 pmid: 15995167 |
| 23. |
Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 2020; 395(10229):1054-62. doi: 10.1016/S0140-6736(20)30566-3.
doi: 10.1016/S0140-6736(20)30566-3 pmid: 32171076 |
| 24. |
Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med 2020; 8(5):475-81. doi: 10.1016/S2213-2600(20)30079-5.
doi: 10.1016/S2213-2600(20)30079-5 pmid: 32105632 |
| 25. | Criner GJ, Connett JE, Aaron SD, et al. Simvastatin for the prevention of exacerbations in moderate-to-severe COPD. N Engl J Med 2014; 370(23):2201-10. doi: 10.1056/nejmoa1403086. |
| 26. |
Truwit JD, Bernard GR, Steingrub J, et al. Rosuvastatin for sepsis-associated acute respiratory distress syndrome. N Engl J Med 2014; 370(23):2191-200. doi: 10.1056/NEJMoa1401520.
doi: 10.1056/NEJMoa1401520 pmid: 24835849 |
| 27. | Zhang XJ, Qin JJ, Cheng X, et al. In-hospital use of statins is associated with a reduced risk of mortality among individuals with COVID-19. Cell Metab 2020; 32(2):176- 87. e4. doi: 10.1016/j.cmet.2020.06.015. |
| 28. | Liu G, Zhang S, Mao Z, et al. Clinical significance of nutritional risk screening for older adult patients with COVID-19. Eur J Clin Nutr 2020; 74(6):876-83. doi: 10.1038/s41430-020-0659-7. |
| 29. |
Deniz O, Gumus S, Yaman H, et al. Serum total cholesterol, HDL-C and LDL-C concentrations significantly correlate with the radiological extent of disease and the degree of smear positivity in patients with pulmonary tuberculosis. Clin Biochem 2007; 40(3-4):162-6. doi: 10.1016/j.clinbiochem.2006.10.015.
doi: 10.1016/j.clinbiochem.2006.10.015 pmid: 17217941 |
| 30. | Ishiyama Y, Gallagher PE, Averill DB, et al. Upregulation of angiotensin-converting enzyme 2 after myocardial infarction by blockade of angiotensin Ⅱ receptors. Hypertension 2004; 43(5):970-6. doi: 10.1161/01.HYP.0000124667.34652.1a. |
| 31. | Dijkman R, Jebbink MF, Deijs M, et al. Replication-dependent downregulation of cellular angiotensin-converting enzyme 2 protein expression by human coronavirus NL63. J Gen Virol 2012; 93(Pt 9):1924-9. doi: 10.1099/vir.0.043919-0. |
| 32. | Putnam K, Shoemaker R, Yiannikouris F, et al. The renin-angiotensin system: A target of and contributor to dyslipidemias, altered glucose homeostasis, and hypertension of the metabolic syndrome. Am J |
| Physiol Hear Circ Physiol 2012; 302(6):H1219-30. doi: 10.1152/ajpheart.00796.2011. | |
| 33. |
Cholesterol Treatment Trialists’ Collaboration. Efficacy and safety of statin therapy in older people: a meta-analysis of individual participant data from 28 randomised controlled trials. Lancet 2019; 393(10170):407-15. doi: 10.1016/S0140-6736(18)31942-1.
pmid: 30712900 |
| 34. |
Lemmers RFH, van Hoek M, Lieverse AG, et al. The anti-inflammatory function of high-density lipoprotein in type II diabetes: A systematic review. J Clin Lipidol 2017; 11(3):712-24. doi: 10.1016/j.jacl.2017.03.
doi: 10.1016/j.jacl.2017.03.013 pmid: 28442299 |
|
013.
doi: 10.1016/j.jacl.2017.03.013 pmid: 28442299 |
|
| 35. | Hui N, Barter PJ, Ong KL, et al. Altered HDL metabolism in metabolic disorders: Insights into the therapeutic potential of HDL. Clin Sci 2019; 133(21):2221-35. doi: 10.1042/CS20190873. |
| 36. |
Wei X, Zeng W, Su J, et al. Hypolipidemia is associated with the severity of COVID-19. J Clin Lipidol 2020; 14(3):297-304. doi: 10.1016/j.jacl.2020.04.008.
doi: 10.1016/j.jacl.2020.04.008 pmid: 32430154 |
| 37. | Guirgis FW, Donnelly JP, Dodani S, et al. Cholesterol levels and long-term rates of community-acquired sepsis. Crit Care 2016; 20(1):1-12. doi: 10.1186/s13054-016-1579-8. |
| 38. | Cirstea M, Walley KR, Russell JA, et al. Decreased high-density lipoprotein cholesterol level is an early prognostic marker for organ dysfunction and death in patients with suspected sepsis. J Crit Care 2017; 38:289-94. doi: 10.1016/j.jcrc.2016.11.041. |
| [1] | 谷雨,张婷,彭敏,施举红. 显微镜下多血管炎患者继发弥漫性肺泡出血和肺间质病的临床特征及预后分析[J]. Chinese Medical Sciences Journal, 2022, 37(4): 293-302. |
| [2] | 林立金, 柳叶茂, 秦娟娟, 雷昉, 汪文鑫, 黄学伟, 刘伟芳, 张兴元, 折志刚, 张鹏, 张晓晶, 金朝霞, 李红良. 1990-2030年全球和区域感染性心内膜炎的疾病负担及其归因危险因素的趋势和预测[J]. Chinese Medical Sciences Journal, 2022, 37(3): 181-194. |
| [3] | 陈紫晗, 赵洲, 邓垂文, 李乃适. 发展中国家空气污染与2型糖尿病的系统评价和Meta分析[J]. Chinese Medical Sciences Journal, 2022, 37(3): 218-227. |
| [4] | 李铁力, 丁海璇, 赵新兰, 罗娟, 陈凯, 唐卓, 黄凌云, 李浪波, 杨丽. MODY3合并肠道神经内分泌肿瘤:1例病例报道[J]. Chinese Medical Sciences Journal, 2022, 37(2): 167-170. |
| [5] | 杜方智, 张瑞丽, 王千秋. 消除梅毒母婴传播:中国在COVID-19大流行前和流行期间的实践经验[J]. Chinese Medical Sciences Journal, 2022, 37(1): 67-72. |
| [6] | 宋兰, 朱振宸, 赵瑞杰, 李鹏昌, 田杜雪, 杜铁宽, 徐燕, 杨启文, 曹玮, 宋伟, 金征宇. 北京市单中心19例COVID-19患者的流行病学特征、影像学表现及临床转归[J]. Chinese Medical Sciences Journal, 2021, 36(2): 85-96. |
| [7] | 吴坤荣, 张恕芳, 关紫菀, 李晓黎, 李蕊, 尹影, 李妍. 亚甲基四氢叶酸还原酶基因C677T多态性与中国2型糖尿病患者冠心病风险增加相关[J]. Chinese Medical Sciences Journal, 2021, 36(2): 103-109. |
| [8] | 祖红林,侯骊坤,刘洪伟,詹渊博,何菊. 应用BITOLA系统筛选腹主动脉瘤与2型糖尿病相互作用的候选基因[J]. Chinese Medical Sciences Journal, 2021, 36(1): 50-56. |
| [9] | 李大胜,王大为,王娜娜,徐海旺,黄河,董建平,夏晨. 北京首例由输入病例导致社区感染的新型冠状病毒肺炎患者:深度学习CT辅助诊断的作用[J]. Chinese Medical Sciences Journal, 2021, 36(1): 66-71. |
| [10] | 林烨, 王祯莲, 严敏, 朱飞雨, 端烨, 孙志琴. 曲美他嗪对糖尿病合并冠心病患者的疗效:一项随机对照试验的荟萃分析[J]. Chinese Medical Sciences Journal, 2020, 35(3): 226-238. |
| [11] | Vahid Damanpak Moghadam,Hamed Shafiee,Maryam Ghorbani,Reza Heidarifar. 新型冠状肺炎患者气管插管的补充建议[J]. Chinese Medical Sciences Journal, 2020, 35(2): 110-111. |
| [12] | 郝秋发, 王宝宝, 张薇, 邱维, 刘倩伶, 李雪梅. 核因子κB抑制剂小白菊内酯改善2型糖尿病肾病肾小管白蛋白摄取[J]. Chinese Medical Sciences Journal, 2020, 35(1): 31-42. |
| [13] | 沈畅, 赵萌, 李芸云, 刘宁朴. 荟萃分析:亚甲基四氢叶酸还原酶基因C677T(MTHFR-C677T)多态性与糖尿病视网膜病变(DR)的关系[J]. Chinese Medical Sciences Journal, 2020, 35(1): 71-84. |
| [14] | 尹影, 李蕊, 李晓黎, 吴坤荣, 李玲, 徐曰东, 廖琳, 杨蕊, 李妍. 伴血脂异常2型糖尿病患者亚甲基四氢叶酸还原酶基因多态性与血浆同型半胱氨酸水平的相关性[J]. Chinese Medical Sciences Journal, 2020, 35(1): 85-91. |
| [15] | 陈强, 张丽伟, 黄党生, 张春红, 王秋霜, 沈东, 熊敏俊, 杨菲菲. 冠状动脉疾病合并糖尿病患者经StentBoost技术指导的经皮冠状动脉介入治疗后5年的随访分析[J]. Chinese Medical Sciences Journal, 2019, 34(3): 177-183. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||
|