Chinese Medical Sciences Journal ›› 2022, Vol. 37 ›› Issue (2): 134-141.doi: 10.24920/003975
• Original Article • Previous Articles Next Articles
Clinical Features of Spontaneous Remission in the Classic Fever of Unknown Origin: A Retrospective Study
Changyi Liu1, Xiaoqing Liu2, 3, 4, Xiaochun Shi2, 3, *( )
)
- 1School of Basic Medicine, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing 100730, China
2Department of Infectious Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing 100730, China
3Centre for Tuberculosis Research, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing 100730, China
4Clinical Epidemiology Unit, International Epidemiology Network, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing 100730, China
-
Received:2021-07-29Accepted:2022-01-11Published:2022-06-30Online:2022-04-26 -
Contact:Xiaochun Shi E-mail:shixch7722@163.com
Cite this article
Changyi Liu, Xiaoqing Liu, Xiaochun Shi. Clinical Features of Spontaneous Remission in the Classic Fever of Unknown Origin: A Retrospective Study[J].Chinese Medical Sciences Journal, 2022, 37(2): 134-141.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks

Figure 1.
Diagnosis and treatment process of classic FUO. FUO: fever of unknown origin; LDH: lactate dehydrogenase; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; Ig: immunoglobulin; CMVDNA: cytomegalovirus DNA; EBVDNA: Epstein-Barr virus; BST: blood serologic test; TB-IGRA: interferon-gamma release assay for Mycobacterium tuberculosis; ANA: antinuclear antibody; ENA: extractable nuclear antigen; ANCA: antineutrophil cytoplasmic antibody; RF: rheumatoid factor; anti-CCP: anti-cyclic citrullinated peptide; CT: computed tomography; PDCs: potential diagnostic clues; SACE: serum angiotensin converting enzyme; TEE: trans esophageal echocardiography; PET/CT: positron emission tomography/computed tomography; NSAIDs: nonsteroidal antiinflammatory drugs."
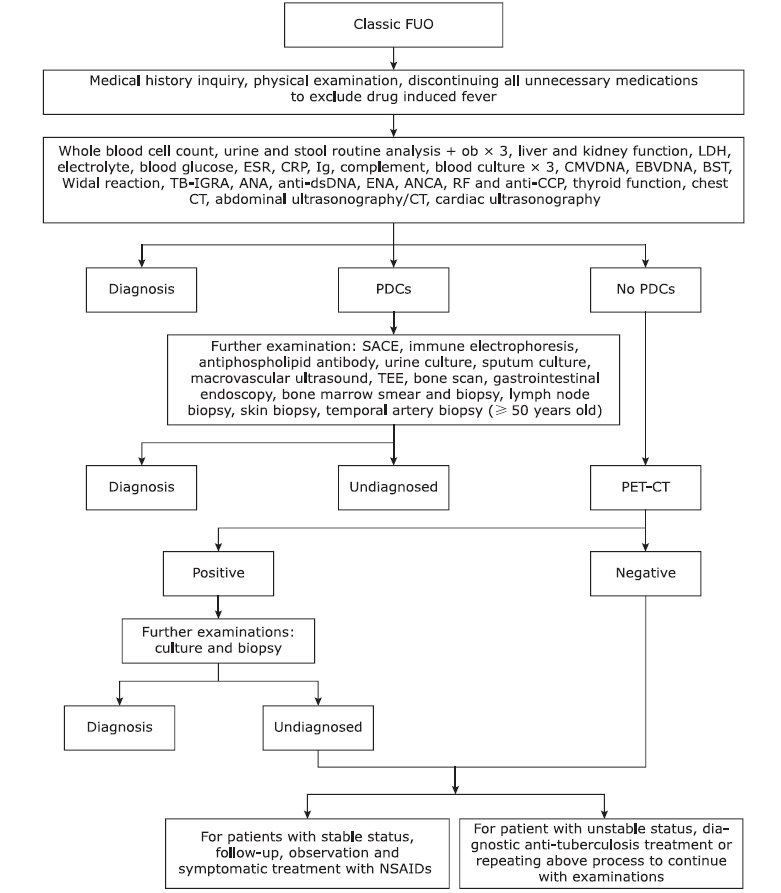
Figure 1.
Table 1.
Etiological diagnosis of 119 classic FUO cases"
| Items | Case number (%) |
|---|---|
| Infectious diseases | 30 (25.2) |
| Bacterial infections | 21 (17.6) |
| Tuberculosis | 8 (6.7) |
| Infective endocarditis | 5 (4.2) |
| Osteomyelitis | 5 (4.2) |
| Disseminated nontuberculous mycobacteria infection | 3 (2.5) |
| Viral infections | 9 (7.6) |
| Epstein-Barr virus infection | 7 (5.9) |
| Cytomegalovirus infection | 2 (1.7) |
| Connective tissue diseases | 28 (23.5) |
| Adult-onset Still’s disease | 16 (13.4) |
| Polymyalgia rheumatica | 3 (2.5) |
| Rheumatoid arthritis | 2 (1.7) |
| Systemic vasculitis | 2 (1.7) |
| Takayasu arteritis | 1 (0.8) |
| Nodular feverish non-suppurative panniculitis | 1 (0.8) |
| Systemic lupus erythematosus | 1 (0.8) |
| Undifferentiated connective tissue diseases | 2 (1.7) |
| Malignant tumors | 8 (6.7) |
| Castleman’s disease | 2 (1.7) |
| Colonic sarcoma | 1 (0.8) |
| Prostate cancer | 1 (0.8) |
| Renal carcinoma | 1 (0.8) |
| Gastric carcinoma | 1 (0.8) |
| Undifferentiated carcinoma | 2 (1.7) |
| Miscellaneous other diseases | 6 (5.0) |
| Hemophagocytic syndrome | 3 (2.5) |
| Necrotizing lymphadenitis | 2 (1.7) |
| Drug induced fever | 1 (0.8) |
| Undiagnosed: follow up results | 47 (39.5) |
| Spontaneous remission | 41 (34.5) |
| Recurrent fever | 6 (5.0) |
Table 1.
Table 2.
Clinical characteristics of classic FUOs with different causes"
| Items | Classic FUO | Spontaneous remission | Infections | Autoimmune diseases | Malignancies | Others | Recurrent FUO |
|---|---|---|---|---|---|---|---|
| n | 119 | 41 | 30 | 28 | 8 | 6 | 6 |
| Age (yrs, mean±SD) | 43±17 | 43±17 | 43±19 | 42±17 | 48±13 | 37±16 | 45±13 |
| Gender [n (%)] | |||||||
| Male | 66 (55.5) | 22 (53.7) | 19 (63.3) | 11 (39.3) | 6 (75.0) | 3 (50.0) | 5 (83.3) |
| Female | 53 (44.5) | 19 (46.3) | 11 (36.7) | 17 (60.7) | 2 (25.0) | 3 (50.0) | 1 (16.7) |
| Tmax [n (%)] | |||||||
| ≤ 39℃ | 41 (34.5) | 15 (36.6) | 12 (40.0) | 7 (25.0) | 4 (50.0) | 2 (33.3) | 1 (16.7) |
| 39°C-41°C | 77 (64.7) | 26 (63.4) | 18 (60.0) | 20 (71.4) | 4 (50.0) | 4 (66.7) | 5 (83.3) |
| > 41℃ | 1 (0.8) | 0 | 0 | 1 (3.6) | 0 | 0 | 0 |
| Rash [n (%)] | 40 (33.6) | 8 (19.5) | 7 (23.3) | 19 (67.9) | 1 (12.5) | 5 (83.3) | 0 |
| Arthritis [n (%)] | 22 (18.5) | 5 (12.2) | 2 (6.7%) | 12 (42.9) | 0 | 1 (16.7) | 2 (33.3) |
| Lymphadenopathy [n (%)] | 45 (37.8) | 10 (24.4) | 10 (33.3) | 17 (60.7) | 2 (25.0) | 4 (66.7) | 2 (33.3) |
| Spleno/hepatosplenomegaly [n (%)] | 51 (42.9) | 12 (29.3) | 15 (50.0) | 13 (46.4) | 2 (25.0) | 4 (66.7) | 3 (50.0) |
| Digestive system involvement [n (%)] | 5 (4.2) | 0 | 1 (3.3) | 0 | 3 (37.5) | 1 (16.7) | 0 |
| Renal involvement [n (%)] | 8 (6.7) | 2 (4.9) | 1 (3.3) | 2 (7.1) | 3 (37.5) | 0 | 0 |
| Respiratory system involvement [n (%)] | 7 (5.9) | 1 (2.4) | 1 (3.3) | 3 (10.7) | 1 (12.5) | 0 | 1 (16.7) |
| Neural system involvement [n (%)] | 5 (4.2) | 1 (2.4) | 3 (10.0) | 1 (3.6) | 0 | 0 | 0 |
| Cardiovascular involvement [n (%)] | 4 (3.4) | 0 | 3 (10.0) | 1 (3.6) | 0 | 0 | 0 |
| WBC (×109/L, mean±SD) | 8.45±4.90 | 6.94±3.84 | 8.26±5.20 | 10.8±5.61 | 10.07±4.28 | 6.60±3.98 | 8.28±4.67 |
| NEUT [×109/L, median (IQR)] | 5.29 (2.96, 7.94) | 3.82 (2.49, 6.28) | 5.26 (2.48, 7.95) | 6.48 (4.69, 12.4) | 6.46 (5.29, 7.84) | 3.86 (2.45, 5.49) | 5.77 (3.23, 10.44) |
| NEUT% (mean±SD) | 69.4±15.3 | 63.8±15.9 | 69.9±17.0 | 75.0±12.4 | 72.9±9.1 | 63.8±15.0 | 80.1±8.1 |
| HB (g/L, mean±SD)a | 108±20 | 112±15 | 110±23 | 103±21 | 92±18 | 110±21 | 112±19 |
| PLT (×109/L, mean±SD)b | 293±132 | 309±116 | 244±150 | 332±114 | 304±145 | 251±70 | 267±198 |
| Anemia [n (%)]a | 70 (60.9) | 19 (51.4) | 18 (60.0) | 19 (67.9) | 7 (87.5) | 4 (66.7) | 3 (50.0) |
| Liver damage [n (%)] | 23 (19.3) | 9 (22.0) | 8 (26.7) | 3 (10.7) | 1 (12.5) | 2 (33.3) | 0 |
| Hypoproteinemia [n (%)] | 65 (54.6) | 20 (48.8) | 18 (60.0) | 15 (53.6) | 7 (87.5) | 3 (50.0) | 2 (33.3) |
| ALB (g/L, mean±SD) | 34±6 | 35±6 | 34±5 | 33±5 | 29±5 | 34±3 | 35±4 |
| ESR (mm/h, mean±SD) | 73±38 | 69±37 | 58±39 | 90±32 | 106±27 | 51±36 | 62±33 |
| CRP [mg/L, median (IQR)] | 56.69 (23.66, 115.55) | 32.40 (17.1, 108.2) | 37.85 (21.64, 97.77) | 91.96 (57.40, 136.55) | 133.56 (73.85, 236.32) | 50.59 (27.63, 83.02) | 46.10 (24.27, 97.98) |
| Ferritin [ng/ml, median (IQR)]c | 551 (253, 1,570) | 380 (103, 601) | 576 (253, 1,675) | 2501 (581, 7,459) | 382 (255, 1,534) | 1126 (567, 3,674) | 272 (101, 445) |
| PET/CT positive [ratio (%)]d | 42/51 (82.4) | 8/12 (66.7) | 9/10 (90.0) | 13/16 (81.3) | 5/5 (100) | 4/4 (100) | 3/4 (75.0) |
| Antibiotic treatment [n (%)] | 116 (97.5) | 40 (97.6) | 30 (100) | 28 (100) | 8 (100) | 5 (83.3) | 5 (83.3) |
| Antivirus treatment [n (%)] | 12 (10.1) | 4 (9.8) | 4 (13.3) | 3 (10.7) | 0 | 0 | 1 (16.7) |
| Diagnostic anti-tuberculosis treatment [n (%)] | 14 (11.8) | 2 (4.9) | 7 (23.3) | 3 (10.7) | 0 | 0 | 2 (33.3) |
| Glucocorticoid treatment [n (%)] | 46 (38.7) | 10 (24.4) | 8 (26.7) | 20 (71.4) | 1 (12.5) | 4 (66.7) | 3 (50.0) |
Table 2.
Table 3.
Univariate analysis of related factors of spontaneous remission in FUO patients"
| Items | Spontaneous remissions in FUO (n=41) | Non-spontaneous remission in FUO (n=78) | OR (95%CI) | P-value |
|---|---|---|---|---|
| Age (yrs, mean±SD) | 43±17 | 43±17 | 1.002 (0.980-1.025) | 0.876 |
| Gender [n (%)] | 0.895 (0.419-1.913) | 0.774 | ||
| Male | 22 (53.7) | 44 (56.4) | ||
| Female | 19 (46.3) | 34 (43.6) | ||
| Rash [n (%)] | 8 (19.5) | 31 (39.7) | 0.426 (0.179-1.015) | 0.054 |
| Arthritis [n (%)] | 5 (12.2) | 17 (21.8) | 0.498 (0.169-1.466) | 0.206 |
| Lymphadenopathy [n (%)] | 10 (24.4) | 35 (44.9) | 0.396 (0.171-0.919) | 0.031 |
| Splenomegaly/hepatosplenomegaly [n (%)] | 12 (29.3) | 37 (47.4) | 0.459 (0.205-1.027) | 0.058 |
| Liver damage [n (%)] | 9 (22.0) | 14 (17.9) | 1.286 (0.503-3.287) | 0.600 |
| WBC (×109/L, mean±SD) | 6.94±3.84 | 9.24±5.22 | 0.892 (0.811-0.981) | 0.019 |
| NEUT [×109/L, median (IQR)] | 3.82 (2.49, 6.28) | 5.93 (3.74, 8.62) | 0.884 (0.794-0.994) | 0.024 |
| NEUT% (mean±SD) | 63.8±15.9 | 72.3±14.3 | 0.967 (0.941-0.995) | 0.018 |
| HB (g/L, mean±SD)a | 112±15 | 106±21 | 1.016 (0.995-1.037) | 0.136 |
| PLT (×109/L, mean±SD)b | 309±116 | 285±139 | 1.001 (0.999-1.004) | 0.331 |
| ALB (g/L, mean±SD) | 35±6 | 33±5 | 1.058 (0.989-1.133) | 0.101 |
| ESR (mm/h, mean±SD) | 69±37 | 74±39 | 0.997 (0.987-1.007) | 0.551 |
| CRP [mg/L, median (IQR)] | 32.40 (17.1, 108.2) | 72.2 (32.2, 117.2) | 0.993 (0.986-1.000) | 0.049 |
| Ferritin [(ng/ml, median (IQR)]c | 380 (103, 601) | 760 (331, 3476) | 1.000 (0.999-1.000) | 0.063 |
| IL-6 [pg/ml, median (IQR)]d | 10.1 (2.0, 21.5) | 21.0 (6.3, 45.2) | 0.980 (0.947-1.014) | 0.244 |
| IL-8 [pg/ml, median (IQR)]d | 58 (42, 120) | 108 (57, 372) | 0.996 (0.990-1.001) | 0.151 |
| IL-10 [pg/ml, median (IQR)]d | 5.0 (5.0, 5.0) | 5.0 (5.0, 10.5) | 0.826 (0.552-1.235) | 0.351 |
| TNF-α[pg/ml, median (IQR)]d | 24.4 (9.2, 39.9) | 25.1 (18.1, 44.2) | 0.979 (0.938-1.023) | 0.343 |
| Lymphocyte [×109/L, median (IQR)]e | 1266 (873, 1629) | 1189 (874, 1720) | 1.000 (0.999-1.000) | 0.482 |
| Lymphocyte percentage [median (IQR)] | 21.2 (15.9, 31.1) | 16.6 (11.5, 23.7) | 1.034 (0.999-1.070) | 0.058 |
| B lymphocyte [×106/L, median (IQR)] | 76 (40, 132) | 65 (42, 105) | 1.002 (0.996-1.007) | 0.508 |
| B lymphocyte percentage [median (IQR)] | 6.9 (3.5, 9.8) | 5.2 (2.8, 8.1) | 1.037 (0.940-1.144) | 0.472 |
| NK cell [×106/L, median (IQR)] | 142 (62, 196) | 116 (61, 194) | 1.001 (0.998-1.005) | 0.407 |
| NK cell percentage [median (IQR)] | 10.7 (6.2, 14.5) | 9.0 (6.4, 13.9) | 1.023 (0.966-1.085) | 0.434 |
| T lymphocyte [×106/L, median (IQR)] | 1042 (712, 1278) | 976 (683, 1329) | 1.000 (0.999-1.000) | 0.338 |
| T lymphocyte percentage [median (IQR)] | 81.6 (77.4, 84.7) | 82.8 (76.2, 88.5) | 0.981 (0.936-1.029) | 0.433 |
| CD4+ T lymphocyte [×106/L, median (IQR)] | 552 (374, 725) | 480 (328, 689) | 1.000 (0.999-1.001) | 0.698 |
| CD4+ T lymphocyte percentage [median (IQR)] | 44.6 (33.8, 50.8) | 43.7 (33.8, 47.9) | 1.017 (0.979-1.057) | 0.383 |
| CD8+ T lymphocyte [×106/L, median (IQR)] | 382 (228, 473) | 356 (238, 647) | 0.999 (0.998-1.000) | 0.189 |
| CD8+ T lymphocyte percentage [median (IQR)] | 29.9 (21.8, 38.9) | 30.7 (24.9, 38.5) | 0.983 (0.948-1.019) | 0.344 |
| CD8+HLA-DR+/CD8+ percentage [median (IQR)] | 45.0 (26.9, 57.6) | 53.8 (32.0, 73.8) | 0.983 (0.965-1.002) | 0.076 |
| CD8+CD38+/CD8+ percentage [median (IQR)] | 67.0 (43.5, 78.8) | 73.1 (55.4, 87.0) | 0.977 (0.956-0.997) | 0.028 |
| PET-CT positive [n (%)]f | 8 (66.7) | 34 (87.2) | 0.294 (0.064-1.350) | 0.115 |
Table 3.
Table 4.
Outcomes of FUO patients undiagnosed at discharge in literatures"
| Study | Number of FUOa | Follow-up time | Patients with spontaneous remission [n (%)] | Deaths [n (%)] |
|---|---|---|---|---|
| Knockaert et al.[ | 61 | 5 years | 41 (67.2) | 6/2b (3.2) |
| Vanderschueren et al.[ | 95 | 574 (125-2052) days | 63 (66.3) | 3 (3.2) |
| Zenone[ | 37 | / | 29 (78.4) | 1 (2.7) |
| Bleeker-Rovers et al.[ | 37 | 12 (6-23) months | 21 (56.8) | 1 (2.7) |
| Mansueto et al.[ | 29 | 2 years | 13 (44.8) | 4 (13.8) |
| Tan et al.[ | 58 | 518 (0.4-830) weeks | 35 (60.3) | 10/9c (15.5) |
Table 4.
| 1. |
Petersdorf RG, Beeson PB. Fever of unexplained origin: report on 100 cases. Medicine (Baltimore) 1961; 40:1-30. doi: 10.1097/00005792-196102000-00001.
doi: 10.1097/00005792-196102000-00001 |
| 2. |
Horowitz HW. Fever of unknown origin or fever of too many origins? N Engl J Med 2013; 368(3):197-9. doi: 10.1056/NEJMp1212725.
doi: 10.1056/NEJMp1212725 |
| 3. |
Shi XC, Liu XQ, Zhou BT, et al. Major causes of fever of unknown origin at Peking Union Medical College Hospital in the past 26 years. Chin Med J (Engl) 2013; 126(5):808-12. doi: 10.3760/cma.j.issn.0366-6999.20121799.
doi: 10.3760/cma.j.issn.0366-6999.20121799 |
| 4. |
Knockaert DC, Dujardin KS, Bobbaers HJ. Long-term follow-up of patients with undiagnosed fever of unknown origin. Arch Intern Med 1996; 156(6):618-20. doi: 10.1001/archinte.156.6.618.
doi: 10.1001/archinte.156.6.618 pmid: 8629872 |
| 5. |
Vanderschueren S, Knockaert D, Adriaenssens T, et al. From prolonged febrile illness to fever of unknown origin: the challenge continues. Arch Intern Med 2003; 163(9):1033-41. doi: 10.1001/archinte.163.9.1033.
doi: 10.1001/archinte.163.9.1033 pmid: 12742800 |
| 6. |
Bleeker-Rovers CP, Vos FJ, de Kleijn EM, et al. A prospective multicenter study on fever of unknown origin: the yield of a structured diagnostic protocol. Medicine (Baltimore) 2007; 86(1):26-38. doi: 10.1097/MD.0b013e31802fe858.
doi: 10.1097/MD.0b013e31802fe858 |
| 7. |
Mansueto P, Carroccio A, Corsale S, et al. Chronic urticaria as a presenting symptom of Crohn’s disease. BMJ Case Rep 2009; 2009:bcr08.2008.0781. doi: 10.1136/bcr.08.2008.0781.
doi: 10.1136/bcr.08.2008.0781 |
| 8. |
Zenone T. Fever of unknown origin in adults: evaluation of 144 cases in a non-university hospital. Scand J Infect Dis 2006; 38(8):632-8. doi: 10.1080/00365540600606564.
doi: 10.1080/00365540600606564 |
| 9. |
Tan Y, Liu X, Shi X. Clinical features and outcomes of patients with fever of unknown origin: a retrospective study. BMC Infect Dis 2019; 19(1):198. doi: 10.1186/s12879-019-3834-5.
doi: 10.1186/s12879-019-3834-5 |
| 10. |
Haidar G, Singh N. Fever of unknown origin. N Engl J Med 2022; 386(5):463-77. doi: 10.1056/NEJMra2111003.
doi: 10.1056/NEJMra2111003 |
| 11. |
Takeuchi M, Nihashi T, Gafter-Gvili A, et al. Association of 18F-FDG PET or PET/CT results with spontaneous remission in classic fever of unknown origin: a systematic review and meta-analysis. Medicine (Baltimore) 2018; 97(43):e12909. doi: 10.1097/MD.0000000000012909.
doi: 10.1097/MD.0000000000012909 |
| 12. |
Nathan C, Ding AH. Nonresolving inflammation. Cell 2010; 140(6):871-82. doi: 10.1016/j.cell.2010.02.029.
doi: 10.1016/j.cell.2010.02.029 pmid: 20303877 |
| [1] | Huizi Gong, Mengyin Wu, Jun Li, Heyi Zheng. The Great Imitator: Atypical Cutaneous Manifestations of Primary Syphilitic Chancre [J]. Chinese Medical Sciences Journal, 2021, 36(4): 279-283. |
| [2] | Pengfei Qu, Baoliang Bai, Ting Duan, Kai Liu, Jinliang Du, Xin Xiong, Penglin Jia, Zhongchun Sun, Puping Lei. Pneumonia, Multiple Pulmonary Infarction and Abscess Caused by a Bamboo Stick Accidentally Piercing into Chest: a Case Misdiagnosed as Pulmonary Tuberculosis [J]. Chinese Medical Sciences Journal, 2021, 36(3): 252-256. |
| [3] | Lianyan Xu, Ke Yan, Le Lu, Weihong Zhang, Xu Chen, Xiaofei Huo, Jingjing Lu. External and Internal Validation of a Computer Assisted Diagnostic Model for Detecting Multi-Organ Mass Lesions in CT images [J]. Chinese Medical Sciences Journal, 2021, 36(3): 210-217. |
| [4] | Lan Song, Zhenchen Zhu, Ruijie Zhao, Pengchang Li, Duxue Tian, Tiekuan Du, Yan Xu, Qiwen Yang, Wei Cao, Wei Song, Zhengyu Jin. Epidemiologic Features, Radiological Findings andClinical Outcomes of 19 Patients with COVID-19in a Single Center in Beijing, China [J]. Chinese Medical Sciences Journal, 2021, 36(2): 85-96. |
| [5] | Dasheng Li,Dawei Wang,Nana Wang,Haiwang Xu,He Huang,Jianping Dong,Chen Xia. An Insight of the First Community Infected COVID-19 Patient in Beijing by Imported Case: Role of Deep Learning-Assisted CT Diagnosis [J]. Chinese Medical Sciences Journal, 2021, 36(1): 66-71. |
| [6] | Wang Xiaolei, Meng Shanshan, Duan Kehang, Hu Yaowei, Wei Feng. Treatment of Retroperitoneal Cavernous Lymphangioma: A Case Report [J]. Chinese Medical Sciences Journal, 2020, 35(3): 283-285. |
| [7] | Wu Ziquan, Zeng Delu, Yao Jiangling, Bian Yangyang, Gu Yuntao, Meng Zhulong, Fu Jian, Peng Lei. Research Progress on Diagnosis and Treatment of Chronic Osteomyelitis [J]. Chinese Medical Sciences Journal, 2019, 34(3): 211-220. |
| [8] | Wang Yingwei, Zhang Xinghua, Wang Botao, Wang Ye, Liu Mengqi, Wang Haiyi, Ye Huiyi, Chen Zhiye. Value of Texture Analysis of Intravoxel Incoherent Motion Parameters in Differential Diagnosis of Pancreatic Neuroendocrine Tumor and Pancreatic Adenocarcinoma [J]. Chinese Medical Sciences Journal, 2019, 34(1): 1-9. |
| [9] | Wang Botao, Liu Mingxia, Chen Zhiye. Differential Diagnostic Value of Texture Feature Analysis of Magnetic Resonance T2 Weighted Imaging between Glioblastoma and Primary Central Neural System Lymphoma [J]. Chinese Medical Sciences Journal, 2019, 34(1): 10-17. |
| [10] | Wang Botao, Fan Wenping, Xu Huan, Li Lihui, Zhang Xiaohuan, Wang Kun, Liu Mengqi, You Junhao, Chen Zhiye. Value of Magnetic Resonance Imaging Texture Analysis in the Differential Diagnosis of Benign and Malignant Breast Tumors [J]. Chinese Medical Sciences Journal, 2019, 34(1): 33-37. |
| [11] | Bai Mingjian, Feng Jing, Liang Guowei. Urinary Myeloperoxidase to Creatinine Ratio as a New Marker for Diagnosis of Urinary Tract Infection [J]. Chinese Medical Sciences Journal, 2018, 33(3): 152-159. |
| [12] | Chen Zhiye, Liu Mengqi, Yu Shengyuan, Ma Lin. Multi-parametric MRI Diagnoses Cerebellar Hemangioblastoma: A Case Report [J]. Chinese Medical Sciences Journal, 2018, 33(3): 188-193. |
| [13] | Dong Dexin, Ji Zhigang, Li Hanzhong, Yan Weigang, Zhang Yushi. Preliminary Application of WCX Magnetic Bead-Based Matrix-Assisted Laser Desorption Ionization Time-of-Flight Mass Spectrometry in Analyzing the Urine of Renal Clear Cell Carcinoma [J]. Chinese Medical Sciences Journal, 2017, 32(4): 248-252. |
| [14] | Li Tao, Zhao Shaohong, Li Jinfeng, Huang Zili, Luo Chuncai, Yang Li. Value of Multi-detector CT in Detection of Isolated Spontaneous Superior Mesenteric Artery Dissection [J]. Chinese Medical Sciences Journal, 2017, 32(1): 28-33. |
| [15] | Ai-chun Liu, Yan-ying Liu, Yan Li, Li Zhang, Zhan-guo Li. Multiple Myeloma Mimicking Spondyloarthritis: a Case Report [J]. Chinese Medical Sciences Journal, 2014, 29(4): 245-247. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
|